Home
 NewsNews
NewsNewsThe World Health Organization releases its first comprehensive, evidence-based global guideline for infertility prevention, diagnosis, and treatment. Addressing one in six people of reproductive age worldwide, the guideline emphasizes equity, human rights, and standardized interventions to improve access to fertility care globally.



The World Health Organization - WHO issues first global guideline on infertility, its comprehensive, evidence-based global guideline for the prevention, diagnosis, and treatment of infertility, cementing fertility care as an integral component of sexual and reproductive health (SRH). The release comes amidst urgent calls to mitigate global inequities in access to fertility care, recognizing infertility as a persistent global public health issue affecting people in all regions and countries.
Developed under the principles of equity, scientific rigour, and respect for human rights, the guideline aims to standardize interventions globally and support countries in delivering high-quality, equitable, and effective health care.
Infertility is defined by WHO as the failure to achieve a pregnancy after 12 months of regular unprotected sexual intercourse. Epidemiological data underscores the necessity of this guideline: approximately one in six people of reproductive age globally experience infertility at some point in their lives, with lifetime prevalence estimated at 17.5%. Crucially, the sources highlight that this prevalence does not differ significantly between high-income countries (HICs) and low- and middle-income countries (LMICs).
As Dr. Tedros Adhanom Ghebreyesus, Director-General of WHO, noted in the foreword, this guideline responds to the urgent need for universally accessible, person-centered services for managing infertility. The guidance is intended primarily for health care professionals (including physicians, embryologists, nurses, and policy-makers) responsible for developing national health policies, services, and financing.

A core foundational element of the new guidelines is the recognition that addressing infertility is central to human rights and global health aspirations. Individuals and couples possess the right to decide the number, timing, and spacing of their children. Infertility can constrain this ability to realize reproductive goals.
The guideline links infertility care directly to the achievement of the right to health, which includes the highest attainable standard of physical, mental, and social well-being. The negative impacts of infertility on mental well-being, relationships, and quality of life, alongside its association with a high prevalence of intimate partner violence, necessitate improved access to prevention, diagnosis, and treatment services.
The WHO emphasizes that addressing infertility is also necessary to enhance equitable access to health care. Access to fertility care remains a significant challenge, largely due to cost barriers in settings without fully funded fertility care. The guideline calls on Member States to establish legislative frameworks, determine eligibility criteria, and facilitate equitable access to safe and effective fertility care, viewing implementation through a public health approach to reduce disparities. Demographic trends, such as declining total fertility rates, should not be used to restrict or deprioritize guideline implementation; rather, the focus must be on supporting individuals and couples in achieving their fertility preferences.
A significant portion of the guideline focuses on proactive strategies for prevention, particularly through education and managing modifiable lifestyle risks.
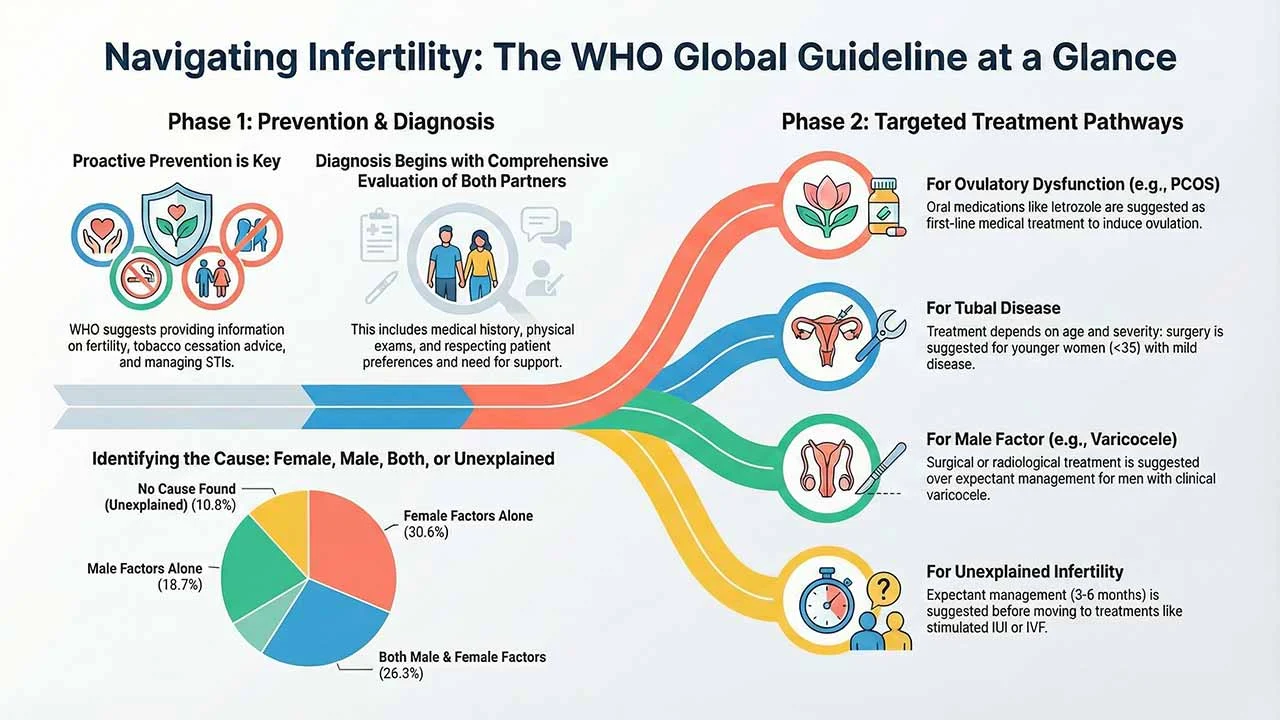
For the general population of reproductive age, WHO suggests providing information about fertility and infertility using low-cost strategies or whenever there is opportunity. This information should be adapted to local contexts and audiences, covering risk factors, lifestyle modifications, age-related fertility decline, and when to seek timely medical consultation. Low-cost settings include schools, primary health care centers, or contraceptive/sexual health clinics.
A major public health intervention strongly recommended is brief advice against tobacco use. WHO recommends that brief advice (30 seconds to 3 minutes) be consistently provided by health care providers as a routine practice to all tobacco users accessing any health care setting. This strong recommendation, adopted from existing WHO guidance, applies directly to individuals and couples planning or attempting pregnancy, given the association between smoking and a higher risk of infertility, especially among women. This advice should follow the 5As: Ask, Advise, Assess, Assist, and Arrange follow-up.
Furthermore, couples and individuals seeking pregnancy should be routinely informed about sexually transmitted infections (STIs), including the significant risk of infertility when STIs are untreated. This is classified as a "Good practice statement" given the evidence of greater prevalence of certain STIs in infertile populations and the potential for untreated infections to cause damage and scarring to reproductive organs.
For individuals already diagnosed with infertility, WHO suggests providing low-cost lifestyle advice (covering diet, alcohol intake, smoking, physical activity, and/or weight management) before and during treatment to optimize pre-pregnancy health.
The guideline provides systematic, evidence-based recommendations for diagnosing the causes of infertility, covering female factors, male factors, and unexplained factors.
General Diagnostic Approach: It is considered good practice that diagnostic tests should be selected based on the clinical findings derived from a comprehensive medical history and physical examination to ensure the evaluation is systematic and cost-effective. This initial consultation should also include listening to individuals and couples, respecting their preferences, and discussing the need for psychosocial or peer support.
Investigation of the male partner is essential, contributing wholly or in part to approximately 45.1% of infertility cases. The guideline addresses the repeatability of semen analysis:
The guidelines offer nuanced conditional recommendations based on the certainty of evidence (often low or very low) for treating different categories of infertility.
Treatment for Ovulatory Dysfunction (PCOS): For women with Polycystic Ovary Syndrome (PCOS) who are unsuccessful with first-line oral therapies (like letrozole or clomiphene citrate with metformin), WHO suggests using gonadotrophins over laparoscopic ovarian drilling (LOD). Although LOD may reduce risks like Ovarian Hyperstimulation Syndrome (OHSS) and multiple pregnancies, gonadotrophins are generally favored as LOD is a surgical procedure with its own risks. If gonadotrophins or other pharmacological therapies fail, WHO suggests using In Vitro Fertilization (IVF) rather than expectant management.
Treatment for Tubal Disease: Treatment decisions concerning tubal disease are stratified by age and severity:
If hydrosalpinx is present in women planning IVF, WHO suggests either salpingectomy or tubal occlusion beforehand, as this condition negatively impacts implantation and IVF success rates. Furthermore, salpingectomy or tubal occlusion is suggested over transvaginal aspiration of hydrosalpingeal fluid before IVF, although aspiration may be offered if surgery is not available or feasible.
Treatment for Uterine Cavity Disorder: For females with infertility and uterine septum who have no history of recurrent pregnancy loss, WHO suggests that hysteroscopic septum resection (septoplasty) not be performed.
Treatment for Male Factors: For men with infertility and semen parameters outside the WHO reference ranges, the Guideline Development Group (GDG) found insufficient evidence to make a recommendation for or against the use of antioxidant supplements.
For men with infertility and clinical varicocele (and semen parameters outside WHO reference ranges), treatment is suggested over no treatment. If treatment is pursued, WHO suggests using either surgical or radiological treatment, with the choice based on factors like feasibility, availability of trained providers, and patient preferences. When surgical treatment is used, microscopic surgery is suggested over other surgical procedures.
Treatment for Unexplained Infertility: Management proceeds in three suggested steps:
Successful implementation requires countries to adapt these recommendations based on local contexts, epidemiological profiles, health system capacity, and sociocultural factors. This includes ensuring that infertility is included in relevant government policies, strategic plans, and financing. Policy-makers are encouraged to consult updated WHO model lists of essential medicines and in vitro diagnostics to facilitate procurement of relevant supplies.
Despite the depth of this first edition, the guidelines acknowledge important research gaps. The GDG noted a deficit in studies from LMICs, a lack of data on patient values, preferences, and acceptability, and suboptimal evidence regarding costs and cost-effectiveness for many interventions. Furthermore, many studies focused on clinical pregnancy rather than the key patient outcome of live birth rate.
Future editions of the guideline are anticipated to expand their scope to address topics currently excluded or limited, such as:
The WHO is encouraging ongoing evidence generation to inform future updates, including tracking developments in artificial intelligence, equipment technology, and medical treatments.
To Access the Guideline, Readers May Visit:
https://www.who.int/publications/i/item/9789240115774



Legacy, North America's leading digital male fertility clinic, has secured New York State CLEP approval for both its semen analysis and DNA fragmentation test – the only mandatory pre-market laboratory review programme in the United States. The approvals confirm clinical-grade validity for at-home samples, extending access to New York patients without a clinic visit.

From 1 July 2026, South Australia's Fertility Treatment Rebate Scheme provides eligible residents with a $250 rebate for pre-treatment testing and a $2,000 rebate for up to two fertility treatment cycles. Backed by an $18.5 million, four-year government commitment, the scheme directly addresses the financial barriers preventing South Australians from accessing fertility care.

apyen, a global leader in male fertility diagnostics, has entered a strategic partnership with My Surrogacy Journey to broaden fertility testing and reproductive health support for intended parents across the United States. The collaboration covers semen analysis, DNA fragmentation testing, and infectious disease screening, with plans for international expansion.

Nucleus Genomics has announced that the Fertility Institute of Hawaii Joins Nucleus IVF+ network, bringing advanced carrier and embryo screening to Hawaii's largest IVF practice. The partnership expands genetic optimization access across the Pacific, with risk reduction data covering endometriosis, heart disease, breast cancer, type 1 diabetes, and Alzheimer's disease.

TFC Taipei Fertility Center has introduced an AI-Powered Embryo Selection model that improves chromosomally normal embryo identification by up to 24%. Presented at ASPIRE 2026, the iDAScore v2.0 system brings precision and objectivity to IVF treatment, reducing implantation failure risk and shortening time to conception for infertile patients.

CDT Equity Inc. (Nasdaq: CDT) has announced the Canadian patent grant for AZD5904 in male infertility, completing approval across all key pharmaceutical target markets. The milestone strengthens CDT's IP position for the AstraZeneca-licensed Myeloperoxidase inhibitor as the company advances active out-licensing and strategic partnering discussions for the asset.

Nucleus Genomics has announced that Nucleus IVF+ joins SCRC, the Southern California Reproductive Center, as part of its rapidly expanding global network. The partnership integrates advanced carrier screening and embryo analysis across SCRC's four California locations, serving thousands of patients annually across Beverly Hills, Santa Barbara, Pasadena, and Ventura.

