Home
 ArticlesArticles
ArticlesArticlesFrozen Egg Thawing survival rates average 80–90% with modern vitrification. Age at freezing is the biggest success factor, younger eggs fertilize better and develop stronger embryos. Banking 10–20 mature eggs improves live birth odds. ICSI remains the gold standard, with blastocyst transfer offering the highest implantation rates.




Egg freezing, medically known as oocyte cryopreservation, has become one of the most powerful tools in modern reproductive medicine. Whether you are delaying parenthood for personal reasons, preserving fertility before cancer treatment, or simply giving yourself more options for the future, understanding what happens after your eggs are frozen is just as important as the freezing process itself.
One of the most common and most important questions patients ask is: "What are the chances my frozen eggs will survive thawing and successfully fertilize?"
The honest answer is it depends, success rates are shaped by several key factors, most notably a woman's age at the time of egg freezing and the number of eggs stored. This guide breaks down everything you need to know, clearly, accurately, and without the medical jargon overload.
When you are ready to use your frozen eggs, whether months or years later, they go through a carefully controlled thawing process called warming. The eggs are removed from cryogenic storage (liquid nitrogen at -196°C) and gently brought back to body temperature using specialized solutions that prevent ice crystal damage to the cell.
Here is what happens step by step:
This process is delicate, science-driven, and requires the skill of an experienced embryology team.

Post-thaw survival rate is the first metric doctors look at. Thanks to a breakthrough technique called vitrification, an ultra-rapid flash-freezing method, survival rates have improved dramatically over the past decade.
Current benchmarks from leading fertility clinics and research data show:
These are population-level averages. Personal outcome will depend on specific factors, especially age at freezing and egg quality.
If there is one thing every fertility specialist agrees on, it is this: the younger you are when you freeze your eggs, the better your outcomes tend to be.
Here is why this matters so profoundly:

Note: These figures represent general estimates. Individual results vary based on clinic, protocol, and patient-specific factors.
The takeaway is clear: egg freezing in your late 20s or early 30s offers the strongest foundation for future success. Freezing at 38 or 40 is still a valid and meaningful option, but it typically requires more eggs and carries lower per-egg odds.
This is one of the most practical questions and one of the most misunderstood. Storing one or two eggs is rarely enough. The number of eggs frozen directly impacts your cumulative success rate.
Fertility specialists generally use these evidence-based benchmarks as a guide:
This is why many women choose to undergo multiple egg-freezing cycles sometimes two or three rounds of ovarian stimulation, to bank enough eggs to feel confident about their chances.
A common misconception is that more eggs always equals better outcomes. While quantity matters, egg quality is the true determinant of success. Two women may each freeze 10 eggs, but if one woman's eggs have higher genetic integrity, her outcomes will almost certainly be superior.
Key markers of egg quality include:
Clinics that offer PGT-A (Preimplantation Genetic Testing for Aneuploidy) allow patients to identify chromosomally normal embryos before transfer, significantly improving implantation rates, particularly for women over 37.
Before vitrification was widely adopted, the older method, slow-freeze cryopreservation, resulted in significantly lower post-thaw survival rates, often below 60%. Ice crystals would form inside cells, damaging the delicate internal machinery.
Vitrification changed everything by:
Today, most leading fertility preservation programs exclusively use vitrification. If you are considering egg freezing, it is worth asking your clinic specifically whether they use vitrification it is the recognized gold standard.
Numbers on paper can feel cold when you are navigating a deeply personal journey. It is important to hold two truths at the same time:
Speaking openly with your reproductive endocrinologist about your personal statistics, not just population averages, is essential. A personalized counseling session that accounts for your AMH levels (anti-Müllerian hormone, a marker of ovarian reserve), antral follicle count, and cycle history gives you a far more accurate picture than any general table.
Before or after egg freezing, these are high-value questions worth bringing to your next appointment:
This content is intended for educational purposes and does not replace personalised medical advice. Always consult a qualified reproductive endocrinologist or fertility specialist for guidance tailored to your individual circumstances.


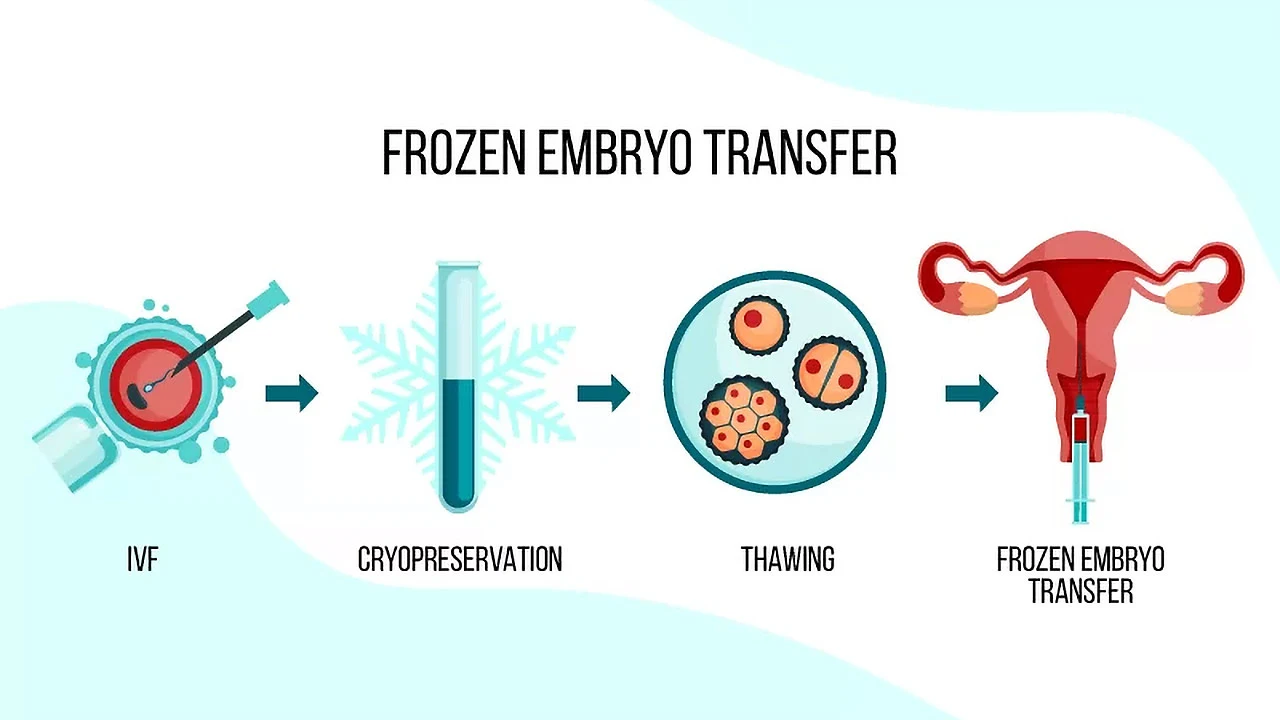
Frozen embryo transfer (FET) is a fertility procedure where previously created and frozen embryos are thawed and placed into the uterus. This comprehensive guide explains the FET process, success rates, benefits, and why it's become a preferred option for many people navigating infertility treatment and building their families.

The vital role of fertility preservation and egg donation in helping women overcome reproductive challenges, allowing them to control their family planning. It highlights how these advancements in reproductive medicine enable women to preserve their fertility and access healthier eggs for future pregnancies.

Egg freezing does not reduce natural fertility or ovarian reserve. This comprehensive guide examines how oocyte cryopreservation works, success rates by age, potential risks including OHSS, costs, and psychological benefits. Facts about preserving reproductive options while maintaining natural conception ability for career-focused and medically indicated fertility preservation.

The best age to freeze sperm and eggs depends on biology, fertility health, and personal choice. Experts recommend egg freezing before 35 and sperm freezing before 40 for stronger outcomes. Advances in technology and lifestyle factors also shape fertility preservation decisions.

Egg freezing allows women to preserve their fertility by extracting, freezing, and storing eggs for future use. Whether postponing parenthood for career, personal reasons, or medical treatments, this comprehensive guide explains the process, costs, success rates, and who should consider this increasingly popular fertility preservation option.
Vitrification vs slow freezing is reshaping ovarian tissue cryopreservation strategies. While slow freezing offers a proven track record, vitrification shows stronger DNA protection and stromal preservation. As fertility preservation advances, clinicians weigh tradition against innovation to improve outcomes for cancer survivors seeking future motherhood.

