Home
 ReportReport
ReportReportIntegrating IVF and Surgical Management in Endometriosis offers a patient-centered strategy to improve fertility while managing chronic pain. By integrating laparoscopic surgery, ovarian reserve assessment, and assisted reproductive technology, clinicians can tailor treatment plans, enhance live birth rates, and optimize reproductive outcomes for women facing complex endometriosis-related infertility challenges.



Endometriosis is a complex, chronic, and often debilitating condition that affects approximately 5% to 10% of women of reproductive age. It occurs when tissue similar to the lining of the uterus, the endometrium, grows outside the uterine cavity, commonly affecting the ovaries, pelvic ligaments, and peritoneum. One of the most significant challenges associated with this condition is its impact on fertility. Research indicates that between 30% and 50% of individuals with endometriosis struggle with infertility, and nearly one-third of all couples seeking help for infertility are found to have the disease.
Managing this condition requires a nuanced approach, often involving a combination of medical, surgical, and assisted reproductive strategies. For many patients, the goal is to find the most effective path to parenthood, which frequently leads to the discussion of IVF and Surgical Management in Endometriosis.

To understand why treatment is necessary, one must first look at how endometriosis disrupts reproduction. The disease is characterized by a multifaceted pathophysiology that interferes with several stages of the reproductive process. These mechanisms include:
While the "retrograde menstruation" theory remains a primary explanation for how the disease begins, suggesting that menstrual blood flows backward through the fallopian tubes, genetic predisposition also plays a role, with a heritability of approximately 50%.
Clinicians use various systems to categorize the severity of the disease. The revised American Society for Reproductive Medicine (rASRM) classification is the most common, staging the disease from Stage I (minimal) to Stage IV (severe) based on the size and location of lesions and adhesions.
However, for patients specifically concerned with fertility, the Endometriosis Fertility Index (EFI) is a more predictive tool. Unlike the rASRM, which only describes the disease at the time of surgery, the EFI integrates surgical findings with clinical factors such as age, years of infertility, and pregnancy history. A score of 10 indicates the highest probability of natural conception post-surgery, while a lower score may suggest that the patient should move more quickly toward assisted reproduction.

A significant hurdle in medical treatment is that most hormonal therapies used to manage endometriosis symptoms, such as oral contraceptives, GnRH agonists, and progestogens, are contraceptive in nature. Consequently, while these are excellent for managing pain, they cannot be used while a patient is actively trying to conceive.
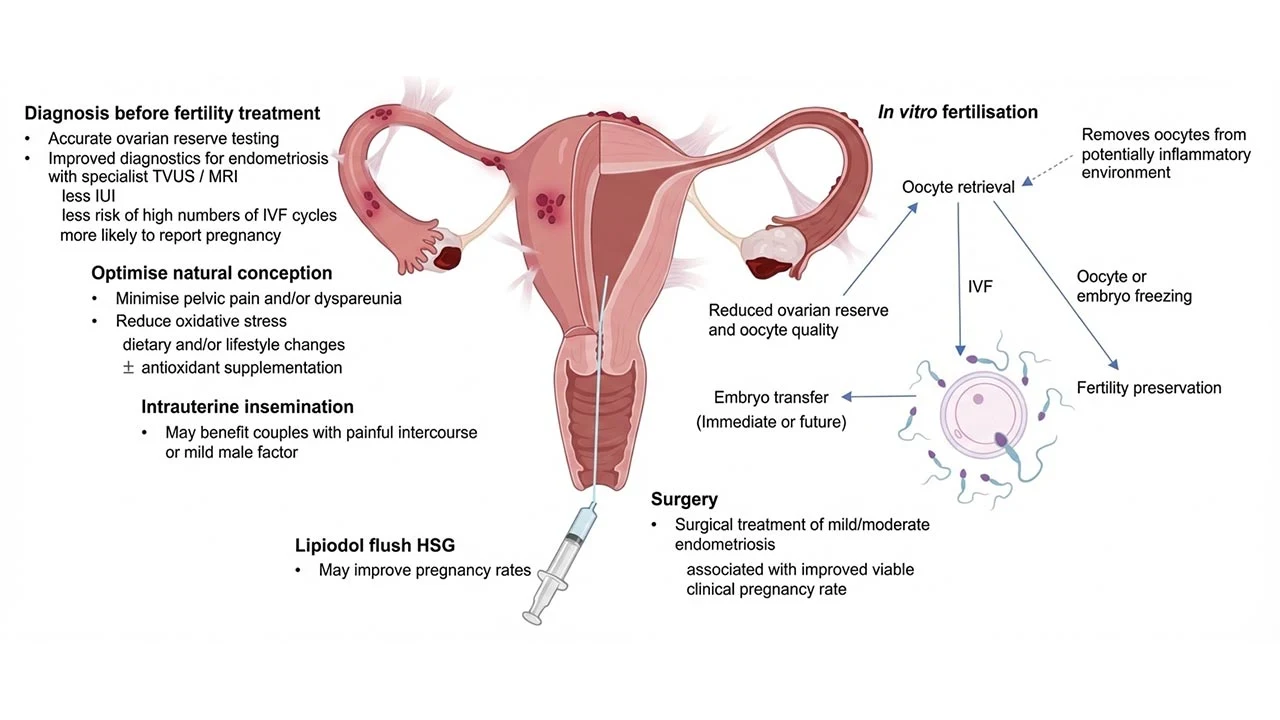
This makes surgery a vital component of the treatment landscape. The primary goal of surgery is to restore normal pelvic anatomy and remove as much of the disease as possible to reduce the inflammatory burden. For patients with minimal-to-mild (Stage I-II) disease, laparoscopic surgery has been shown to improve spontaneous pregnancy rates, though the evidence remains somewhat conflicting.
For more advanced stages (III-IV), surgery is often considered when the patient is symptomatic, particularly when experiencing chronic pelvic pain. However, surgery carries risks, including the formation of new adhesions and the potential to reduce the ovarian reserve if healthy ovarian tissue is inadvertently removed during the excision of an endometrioma. This delicate balance highlights the importance of expert consultation when discussing IVF and Surgical Management in Endometriosis.
When natural conception or surgery is not successful or appropriate, In Vitro Fertilization (IVF) becomes a mainstay of treatment. IVF is particularly effective because it partially bypasses distorted pelvic anatomy and tubal disease.
Evidence suggests that IVF outcomes for individuals with Stage I and II endometriosis are comparable to those without the disease. While patients with Stage III and IV disease may see a reduction in the number of oocytes (eggs) retrieved and lower live birth rates per cycle, IVF remains a highly appropriate and effective indication for these individuals.
A vital factor in the success of ART is timely diagnosis. Many patients experience a diagnostic delay of up to a decade. Studies show that patients who are diagnosed with endometriosis before starting ART have higher live birth rates and require fewer cycles than those who remain undiagnosed during their initial fertility treatments. Furthermore, patients can be reassured that undergoing ovarian stimulation for IVF does not appear to exacerbate endometriosis symptoms or lead to disease progression.
The most modern approach to treatment involves a holistic integration of strategies. While surgery can treat pain and potentially improve the pelvic environment, ART offers a more direct route to pregnancy when time is of the essence, particularly for older patients or those with a low ovarian reserve.
Currently, international guidelines from ESHRE and ASRM do not recommend undergoing surgery solely to improve the outcomes of a subsequent IVF cycle. Instead, the decision must be patient-centered and individualized. Factors that influence the integration of IVF and Surgical Management in Endometriosis include:
The journey toward parenthood for those with endometriosis is rarely a straight line. It requires balancing the need for symptom relief with the urgent goals of fertility. While surgery remains a powerful tool for restoring anatomy and alleviating pain, IVF provides a critical solution for overcoming the biological hurdles posed by the disease.
The integration of IVF and Surgical Management in Endometriosis allows for a tailored treatment plan that respects the patient's unique clinical scenario, reproductive goals, and personal preferences. By utilizing tools like the EFI and prioritizing early diagnosis, clinicians and patients can work together to optimize the chances of a successful pregnancy while effectively managing this chronic condition. Ultimately, a holistic approach that considers both the physical disease and the patient's broader life goals is essential for the best possible outcomes.



The University of Aberdeen has launched a redesigned, free IVF success calculator, the OPIS tool, powered by updated national HFEA data. Built with patients at its centre, the IVF success calculator provides tailored success estimates across up to six IVF or ICSI cycles, helping couples plan emotionally, physically, and financially.

A retrospective cross-sectional study of 276 ART patients suggests that the oestradiol-to-oocyte ratio (EOR) could serve as a meaningful prognostic marker for IVF outcomes in PMOS. The research examines EOR across four categories, incorporating subgroup analysis by luteinising hormone activity during ovarian stimulation.

AutoIVF's OvaReady device is advancing IVF egg retrieval technology by recovering "stealth oocytes" from discarded follicular fluid. With Northeastern University co-op students Tori Christianson and Jake Percival refining its prototypes, the Natick, Mass, based startup is preparing for clinical trials, aiming for FDA clearance to improve IVF success rates.
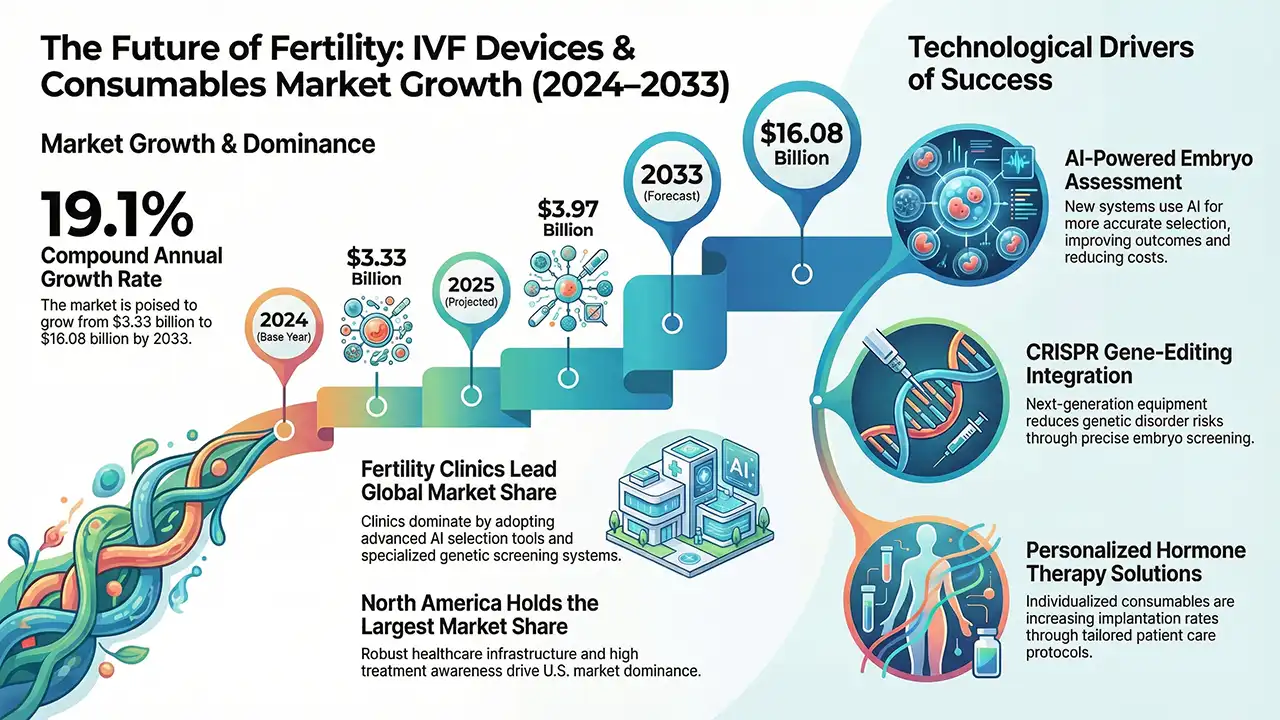
The global IVF Devices and Consumables market is projecting a significant surge to $16.08 billion by 2033. Driven by rising infertility and tech innovations, the analysis covers regional shifts, product segments, and emerging trends, highlighting the industry’s evolution alongside the growing Smart Fertility Tracker Market
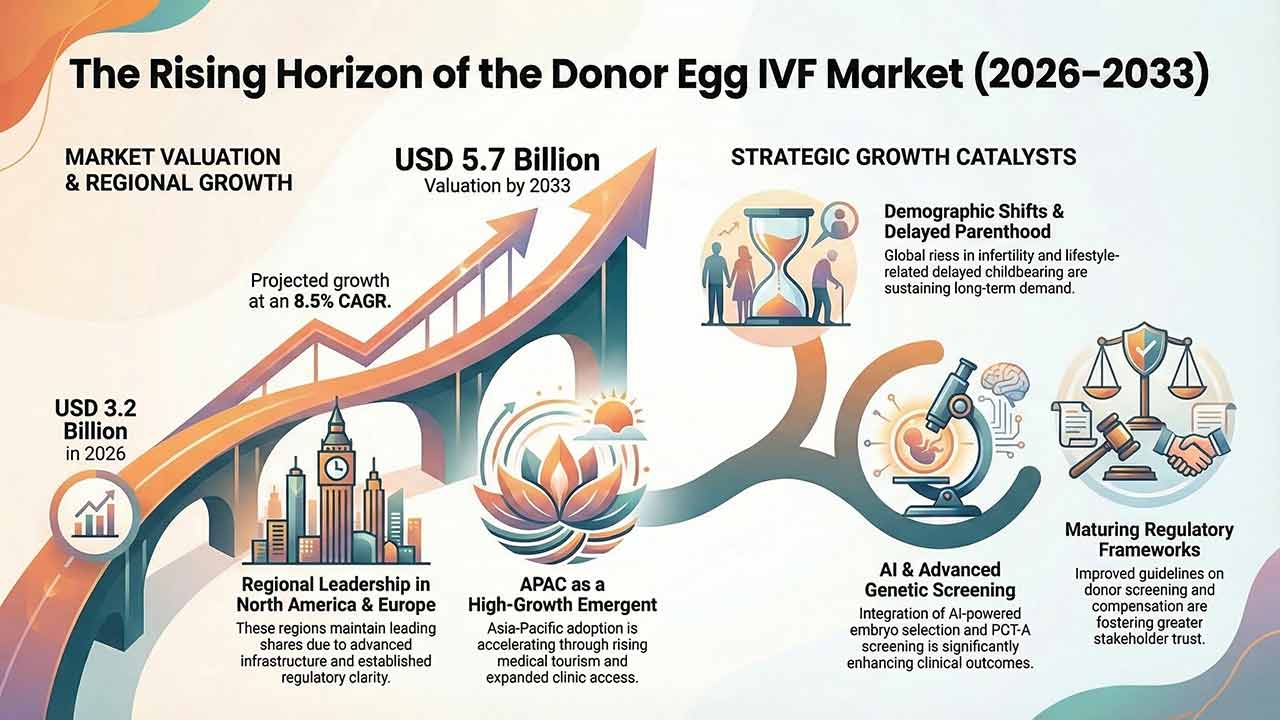
This comprehensive analysis examines the global Donor Egg IVF market, forecasting a valuation of USD 5.7 billion by 2033. The report explores critical growth drivers, including delayed parenthood, technological breakthroughs in embryo selection, and shifting regulatory landscapes, offering a detailed breakdown of market segmentation and regional growth trajectories for the next decade.

Global Preimplantation genetic testing market outlook covering growth drivers, segmentation, regional trends, key technologies, restraints, opportunities, and competitive landscape approaching $1B by 2032.

