Home
 NewsNews
NewsNewsNew clinical evidence reports the birth of healthy twins after aneuploid embryo transfer, highlighting how PGT-A results can differ from developmental outcomes. The case underscores the complexity of embryo biology and the need for careful, individualized interpretation of genetic screening within modern IVF practice in fertility clinics worldwide.



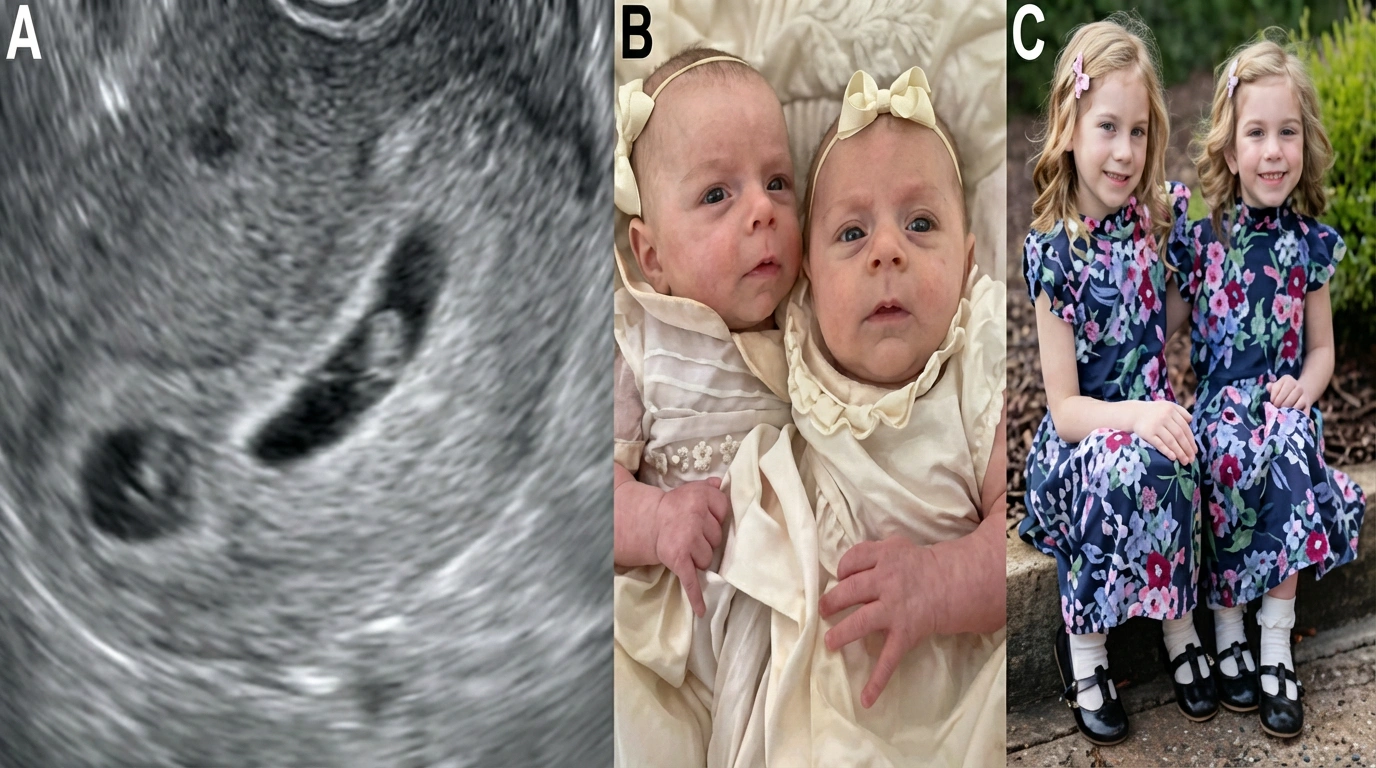
A newly published clinical case has documented the birth of healthy twins following aneuploid embryo transfer, contributing important evidence to the growing understanding of how preimplantation genetic testing for aneuploidy functions in real-world IVF settings. The case, published in Fertility and Sterility, details how two embryos labelled as aneuploid after trophectoderm biopsy went on to implant and ultimately resulted in the birth of chromosomally normal twins. The outcome of this highlights how complex early embryo development can be and why genetic screening results require careful, case-by-case interpretation in fertility care.
The patient underwent IVF with PGT-A, during which two blastocysts were identified as aneuploid based on a small trophectoderm cell sample. After counseling, the decision was taken to move forward with aneuploid embryo transfer, and both embryos were transferred. The pregnancy advanced without any complications, and the patient delivered healthy twins with no structural abnormalities. Postnatal karyotyping later authenticated that both infants had normal chromosomal profiles. The case illustrates how PGT-A embryo viability assessment, while valuable, is not absolute and must be contextualized within the biology of early embryonic development.
From a clinical perspective, the findings reinforce established knowledge that a trophectoderm biopsy represents only a limited portion of the embryo and does not sample the inner cell mass, which forms the fetus. Variability in early cell division, mosaicism, and lineage allocation can lead to discrepancies between biopsy findings and developmental outcomes. Increasingly, research suggests that some embryos labelled as aneuploid may still retain the capacity for normal development, either because chromosomal abnormalities are confined to placental tissue or because normal cell populations predominate as development progresses. This biological flexibility is a key consideration when evaluating outcomes following aneuploid embryo transfer.
Importantly, the authors do not suggest that embryos diagnosed as aneuploid should be transferred routinely. Instead, the case points to the need for better counselling and continued research into how genetic findings are used when making clinical decisions. From the perspective of fertility clinics and IVF laboratories, the case underscores the importance of interpreting PGT-A results together with embryo morphology, patient history, and the broader clinical picture. As IVF continues to evolve, cases like this are guiding embryo selection toward a more careful, evidence-based, and individualized approach.



India's Central Drugs Standard Control Organisation has overhauled CDSCO IVF reagent sale norms, directing that all ART media, culture solutions, and reagents be supplied exclusively to clinics registered under the ART (Regulation) Act and Surrogacy (Regulation) Act. The move targets a growing unlicensed supply chain feeding an estimated 40–50% of India's 2,000-plus IVF centres.

Abu Dhabi University and FertiClinic Group have joined forces to establish the FertiClinic Reproductive Research Lab, an advanced reproductive research lab in Abu Dhabi housing IVF, andrology, and cryopreservation facilities. The partnership supports UAE national priorities, bridges academic and clinical expertise, and advances fertility innovation across the region.

NHS Kent and Medway has overhauled its fertility funding policy in a move that sees NHS cuts IVF access for thousands of patients. Effective 1 April 2026, the eligible age ceiling drops from 40 to 38, funded cycles fall from two to one, and embryo transfers are capped at two.

ASEAN's First Telemedicine IVF by Inspire IVF introduces a new era of remote fertility care. Combining AI technology with expert consultation, the platform enables global access, real-time monitoring, and personalised treatment planning, positioning Thailand as a leading hub for fertility services and advancing digital transformation in reproductive healthcare.

CSG.BIO has gone ahead with the acquisition of Hanabusa IVF, Asian Egg Bank, thereby making it a world leader in reproductive medicine and cutting-edge clinics with enhanced patient reach and advanced laboratory capabilities.

Wisconsin lawmakers from both parties are proposing bills to reduce IVF treatment costs. Republicans suggest a $5,000 tax credit for expenses, while Democrats want mandatory insurance coverage. With IVF cycles costing $20,000-$30,000 and 170,000 residents facing infertility, both parties seek affordable solutions through different approaches.

The AI-specialized Infertility Center, which is the largest in Asia, is open in Magok, Seoul and has begun its full-scale medical services from November 17 thereby marking the new era when it comes to fertility in the region.

