Home
 ArticlesArticles
ArticlesArticlesGuidance on why first IVF cycles fail, how to adjust protocols, when to consider donor gametes or PGT-A, and how to plan emotionally and financially for retries to improve cumulative success.




When the first IVF cycle fails, the next steps begin with a sober truth, even well-executed cycles can miss, and the path to a live birth is often cumulative, not linear. The second truth is just as important: recalibrating strategy clinically, emotionally, and financially meaningfully improves the odds on subsequent attempts.
Most unsuccessful cycles trace back to an interplay of embryo competence and uterine receptivity, with age as a powerful modifier of both. Embryo aneuploidy rises with maternal age, while endometrial receptivity can also shift with aging and uterine pathology, producing a dual headwind for implantation.
Starts with a structured debrief: confirm embryo grading and developmental kinetics, audit stimulation and trigger timing, assess endometrial preparation and timing, and review semen parameters and lab methods. This level of rigor distinguishes one-off bad luck from systematic issues that can be fixed.
Evidence supports a stepwise re-assessment after one failed transfer, reserving the “recurrent implantation failure” label for multiple well-controlled failures while still acting early on modifiable risks. A targeted workup can surface endometrial, immunologic, or anatomic factors and align the next cycle to patient-specific biology.
Emphasizes that cumulative probability rises across well-designed cycles, provided each iteration learns from the last rather than simply repeating it. Audited iteration is a strategy, not a fallback.
Donor oocytes dramatically improve outcomes for patients where embryo quality is constrained by age-related aneuploidy or repeated poor blastulation, because the limiting factor shifts from oocyte competence to uterine readiness. The decision is personal and clinical, but for many, donor eggs convert stalled probability into an actionable plan.
Include donor options early in counseling so time-sensitive patients can compare probable timelines and cumulative live birth trajectories side-by-side. This transparency respects both biology and budgets.
Preimplantation genetic testing for aneuploidy can reduce transfers spent on visibly normal but chromosomally abnormal embryos, yet its overall effect on live birth varies by age and prognosis. For favorable-prognosis patients, randomized and health-technology assessments show no clear live birth advantage, while in women ≥35–38 it may reduce miscarriage or increase per-transfer success at the cost of fewer transferable embryos and time.
PGT-A as a tool that sorts embryos, not as a universal escalator to higher cumulative live birth; its benefits are situational and must be balanced against opportunity cost.
For some patients, especially those with low ovarian reserve or those seeking less medication burden, natural or mild stimulation IVF can preserve quality while lowering cost, albeit often producing fewer embryos. Emerging evidence suggests cumulative live birth can be comparable to conventional stimulation when cycles are repeated efficiently.
When the first IVF cycle fails, shifting to mild or natural approaches to enable multiple faster cycles, particularly when high-dose stimulation has not yielded qualitatively better embryos. This is a tempo change designed for sustainability.
A “cycle aggregator” model organizes several planned retrievals or rapid-repeat cycles to build an embryo cohort before transfers, especially valuable when each individual cycle yields few oocytes. By front-loading retrievals and batching analysis and transfer decisions, couples gain selection latitude without losing calendar time.
This approach reframes success as the probability across a cluster of optimized cycles, rather than as a judgment based on a single outcome. This mindset aligns medical tactics with statistical reality.
ICSI is indispensable when fertilization is at risk, but using ICSI without indication can paradoxically lower live birth by reducing viable oocytes available; matching method to indication matters. Couples should consider DNA fragmentation testing, varicocele assessment when relevant, antioxidant and lifestyle optimization, and testicular sperm retrieval in select high-fragmentation contexts.
Include a male-factor audit in every debrief because the competence of an embryo is a result of the biology of both gametes, not just the ovary.
Failed treatment is a profound emotional event; structured support protects decision quality on the next cycle. Counseling, peer groups, and scheduled “decision breaks” reduce distress, improve adherence, and help couples negotiate donor options or protocol changes without regret.
When First Treatment Doesn’t Work: Next Steps and Alternatives should make emotional care standard, not optional; clarity under stress is a clinical asset as much as a personal one.
Financial planning is a clinical enabler because the best plan is moot if funding collapses mid-course. Compare per-cycle costs to cumulative packages, weigh the economics of PGT-A and cryopreservation, and consider whether mild or natural cycles enable more attempts within the same budget while preserving quality.
The financial strategy for retries aligns medical iteration with a financial runway, enabling patients to execute their chosen plan, not just initiate it. This alignment is central to sustained progress.
Translating lessons into action yields momentum and confidence for patients and teams. A concise, outcome-oriented checklist can structure the next attempt and shorten time to a successful transfer.
When next steps are specific, scheduled, and grounded in the couple’s values, clinical evidence guides the path, but preferences set the pace. This combination makes setbacks survivable and progress tangible.
When First Treatment Doesn’t Work: Next Steps and Alternatives is not a consolation; it is a blueprint for improving probability through calibrated iteration. By clarifying why cycles fail, tailoring protocols across stimulation, lab, and timing, using donor options and PGT-A judiciously, and underwriting the plan with emotional and financial preparedness, most couples convert early disappointments into cumulative success.
When First Treatment Doesn’t Work: Next Steps and Alternatives, followed with discipline, transforms uncertainty into a series of bounded, data-informed decisions; and in fertility care, a series is often what delivers the outcome that a single attempt could not.



Advanced female age causes fertility decline through reduced egg quantity, increased chromosomal abnormalities, and mitochondrial dysfunction. Understanding these biological mechanisms helps women make informed family planning decisions. Modern fertility treatments including IVF, preimplantation genetic testing, and egg freezing offer practical solutions to overcome age-related reproductive challenges when trying to conceive.
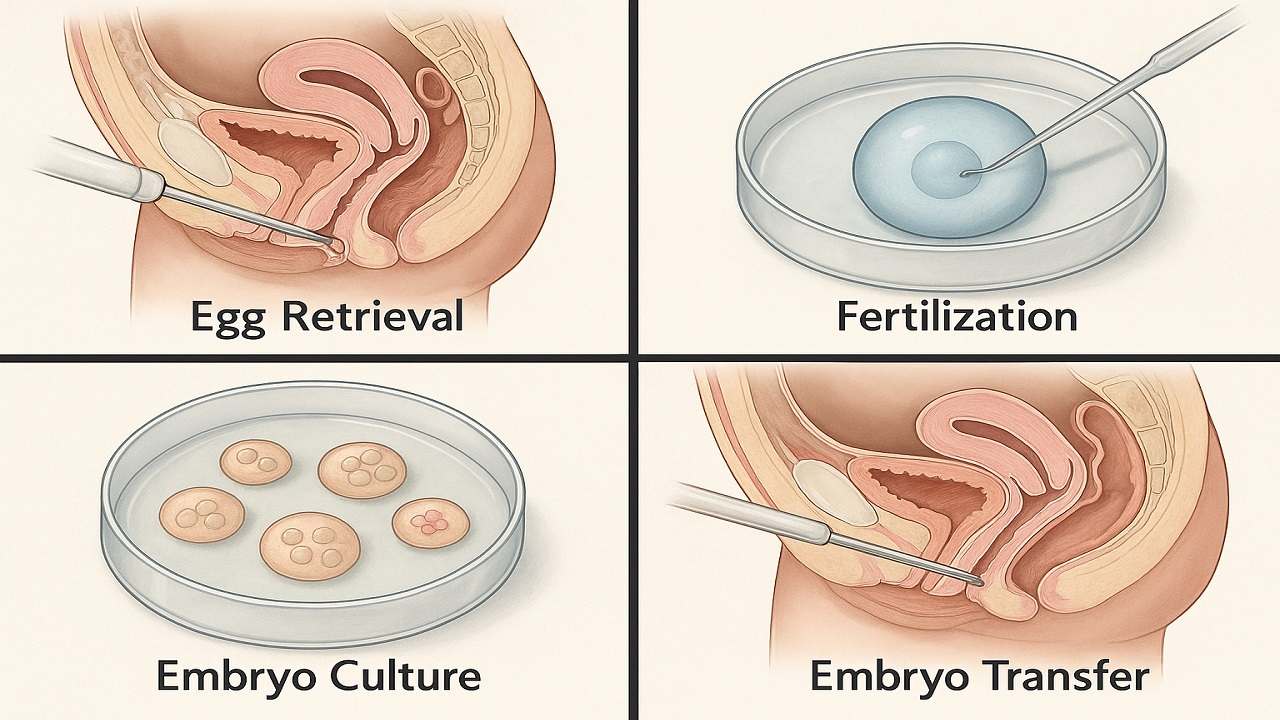
In Vitro Fertilization (IVF) process step by step, emphasising the importance of various stages such as ovarian stimulation, egg retrieval, fertilization, and embryo transfer in maximising the In Vitro Fertilization (IVF) Success Rate. It highlights how a thorough understanding of the procedure can prepare couples and individuals for their In Vitro Fertilization(IVF) journey, ultimately improving their chances of achieving a successful pregnancy.

Vitamin D Deficiency Affect IVF outcomes by influencing endometrial receptivity, embryo quality, and hormone balance. Clinical evidence, age-specific risks, and PCOS implications, while offering actionable strategies to optimize Vitamin D levels and improve IVF success rates and pregnancy outcomes in a structured, patient-focused approach.

Preimplantation Genetic Testing (PGT) revolutionizes IVF by screening embryos for chromosomal abnormalities and genetic disorders before transfer. This advanced technology increases pregnancy success rates, reduces miscarriage risk, prevents inherited diseases, and shortens time to pregnancy while providing diagnostic clarity and reducing emotional stress for couples.

Clinical evidence increasingly demonstrates that emotional stress or grief reduces the chances of IVF success through sophisticated biochemical pathways that directly influence reproductive physiology. This relationship extends far beyond simple correlations, revealing profound mechanistic connections between psychological distress and the delicate orchestration of hormonal events essential for successful conception.
IVF in 2025 is shifting from hype to evidence-based innovation. As precision, automation, AI, and genetic advances reshape fertility care, patients must distinguish proven breakthroughs from outdated add-ons. This guide examines five groundbreaking IVF technologies in 2025 to understand which advances genuinely improve outcomes

Managing Recurrent Implantation Failure (RIF) outlines evidence-based diagnostics and treatment pathways to improve IVF success rates, emphasizing clarity, cautious use of add-ons, and realistic patient expectations.

