Home
 ArticlesArticles
ArticlesArticlesVitrification vs slow freezing is reshaping ovarian tissue cryopreservation strategies. While slow freezing offers a proven track record, vitrification shows stronger DNA protection and stromal preservation. As fertility preservation advances, clinicians weigh tradition against innovation to improve outcomes for cancer survivors seeking future motherhood.



In the rapidly evolving world of reproductive medicine, the focus has shifted significantly toward not just surviving life-threatening illnesses but ensuring a high quality of life afterward. For many women, this means preserving the possibility of biological motherhood. As cancer survival rates have increased by more than 1.6% over the last several years due to better diagnostics and therapies, the side effects of these life-saving treatments, specifically gonadotoxic chemotherapy and radiation, have become a major concern. These treatments can lead to premature ovarian failure, stripping away both the ability to produce hormones and the ability to conceive.
Ovarian Tissue Cryopreservation (OTC) has risen as a beacon of hope in this context. Unlike more common methods like freezing eggs or embryos, which require weeks of hormonal stimulation that many cancer patients cannot afford to wait for, OTC involves surgically removing and freezing strips of the ovarian cortex. While once considered an experimental approach, it is now becoming a clinical reality, with a worldwide live birth rate estimated between 30% and 70%, resulting in more than 70 babies born to date. As this technology moves into the mainstream, the medical community is deeply engaged in a technical evolution, determining the most effective way to "pause" the biological clock through the lens of Vitrification vs slow freezing.
For several decades, slow freezing was the undisputed gold standard for preserving human ovarian tissue. This method relies on a controlled, gradual reduction in temperature, often using specialized, high-tech equipment to ensure the cooling rate is perfectly managed. The underlying philosophy of slow freezing is to allow water to leave the cells slowly and predictably. By doing so, the method seeks to prevent the formation of large, jagged ice crystals that can pierce delicate cellular membranes like microscopic shards of glass.
Historically, slow freezing has a significant advantage, a proven track record. The vast majority of live births resulting from ovarian tissue transplantation have utilized tissue preserved via this traditional method. However, the technique is not without its biological costs. Because the process is so gradual, the tissue is exposed to fluctuating temperatures for a longer duration, which can lead to a phenomenon known as "chilling injury." Additionally, some studies indicate that slow freezing might result in a significant decrease in the number of follicles and can harm the ovarian stroma, which is the important tissue that supports the developing follicles.
As technology progressed, a newer, ultra-rapid cooling technique known as vitrification emerged as a powerful alternative. Rather than slowly lowering the temperature, vitrification effectively "flash-freezes" the tissue, turning it into a glass-like solid state in a matter of seconds. This process bypasses the crystallization phase entirely, meaning that no ice crystals are formed within the cells.
The technical differences in Vitrification vs slow freezing are stark. While slow freezing uses lower concentrations of cryoprotectants over a long period, vitrification requires much higher concentrations of these chemicals to achieve its "glassy" state almost instantly. This method is lauded for being time-saving, technically simple, and far more cost-effective because it does not require expensive, programmable freezing machinery. However, the high concentration of cryoprotectants presents its challenge, if the tissue is exposed to these chemicals for too long or at the wrong temperature, they can become toxic to the very cells they are meant to protect.
The primary goal of any cryopreservation method is to keep the primordial follicles alive and healthy. These follicles are the "seeds" of future life, making up more than 90% of the ovarian reserve in the preserved tissue. When experts compare the structural outcomes of Vitrification vs slow freezing, the visual results are often surprisingly similar. In most cases, both methods are highly effective at maintaining the basic shape and appearance of these follicles.
Under a microscope, a follicle preserved through slow freezing and one preserved through vitrification might look identical. Both techniques generally preserve the proportion of morphologically intact follicles at comparable rates. However, modern reproductive science has learned that looking healthy is only half the battle. A follicle can appear intact but may have sustained underlying damage that prevents it from ever developing into a mature egg.
The real difference between the two methods often lies at the molecular level. One of the most critical indicators of a follicle's future potential is its genetic integrity. Even if a follicle looks perfect, it may be undergoing "apoptosis," a process of programmed cell death often triggered by cellular stress during the freezing process.
This is where the debate over Vitrification vs slow freezing takes a significant turn. Research has indicated that vitrification is often associated with significantly less DNA fragmentation within the primordial follicles compared to the traditional slow-freezing method. By avoiding the formation of ice crystals and the mechanical stress of slow cooling, vitrification appears to offer a gentler environment for the delicate strands of DNA. Lower levels of DNA damage suggest that follicles preserved through vitrification may have a better chance of surviving the "thaw" and successfully developing into primary or secondary follicles once they are transplanted back into the body.
While the follicles are the stars of the show, they cannot survive without a healthy supporting cast. The ovarian stroma is a complex network of blood vessels, nerves, and connective tissue that provides the necessary environment for follicles to grow. When ovarian tissue is transplanted, the body must quickly restore blood flow to the area, a process called revascularization, to keep the follicles alive.
The preservation of the ovarian stroma is a critical battleground in the Vitrification vs slow freezing comparison. Evidence suggests that vitrification is markedly superior at protecting these supportive stromal cells. When the stroma is well-preserved, it provides a more stable and nutrient-rich "soil" for the follicles. This enhanced preservation is believed to lead to improved ovarian function and a faster restoration of hormonal activity after the tissue is grafted back into the patient.
If vitrification offers better DNA protection and superior stromal preservation, why hasn't it completely replaced slow freezing? The answer lies in the complexity of the human ovary. Unlike a single embryo or egg, the ovary is a dense organ composed of many different types of cells, each with its own "diffusion rate" for cryoprotectants.
Because there is currently no single standardized protocol for vitrification, different clinics use various "cocktails" of protective chemicals and different exposure times. For example, the time the tissue spends in an "equilibration solution" before the final flash-freeze can significantly impact how well the stromal cells survive. This lack of standardization means that while the potential of vitrification is higher, the results can be more variable depending on the specific protocol used.
As the field of fertility preservation matures, clinicians are looking beyond just the method of freezing. Some are now exploring a "dual approach" that combines the best of both worlds. At the time of tissue removal, small "antral follicles" can be harvested separately. The immature eggs inside these follicles can then be matured in a lab, a process called in vitro maturation (IVM) and frozen individually. This gives a woman two chances at motherhood, the transplanted tissue and the individually frozen eggs.
Ultimately, the choice between Vitrification vs slow freezing involves weighing the long-term track record of traditional methods against the biological promises of modern ultra-rapid cooling. While slow freezing has brought dozens of babies into the world, the biological advantages of vitrification, particularly regarding DNA health and stromal support, make it an incredibly compelling choice for the future of the field.
The journey from a cancer diagnosis to the birth of a healthy child is a long and difficult road, but the advancements in Ovarian Tissue Cryopreservation are making that journey possible for more women every year. While the debate over the "best" method continues, it is clear that both techniques have moved the needle from experimental science to life-changing medicine.
As protocols continue to evolve, the distinction between Vitrification vs slow freezing will become the cornerstone of personalized fertility preservation strategies. By refining these techniques, scientists are not just freezing cells; they are preserving hope, autonomy, and the future dreams of countless women worldwide. The choice of method may change as more data emerges, but the goal remains steadfast, ensuring that a medical crisis today does not dictate the family possibilities of tomorrow.



Frozen Egg Thawing survival rates average 80–90% with modern vitrification. Age at freezing is the biggest success factor, younger eggs fertilize better and develop stronger embryos. Banking 10–20 mature eggs improves live birth odds. ICSI remains the gold standard, with blastocyst transfer offering the highest implantation rates.
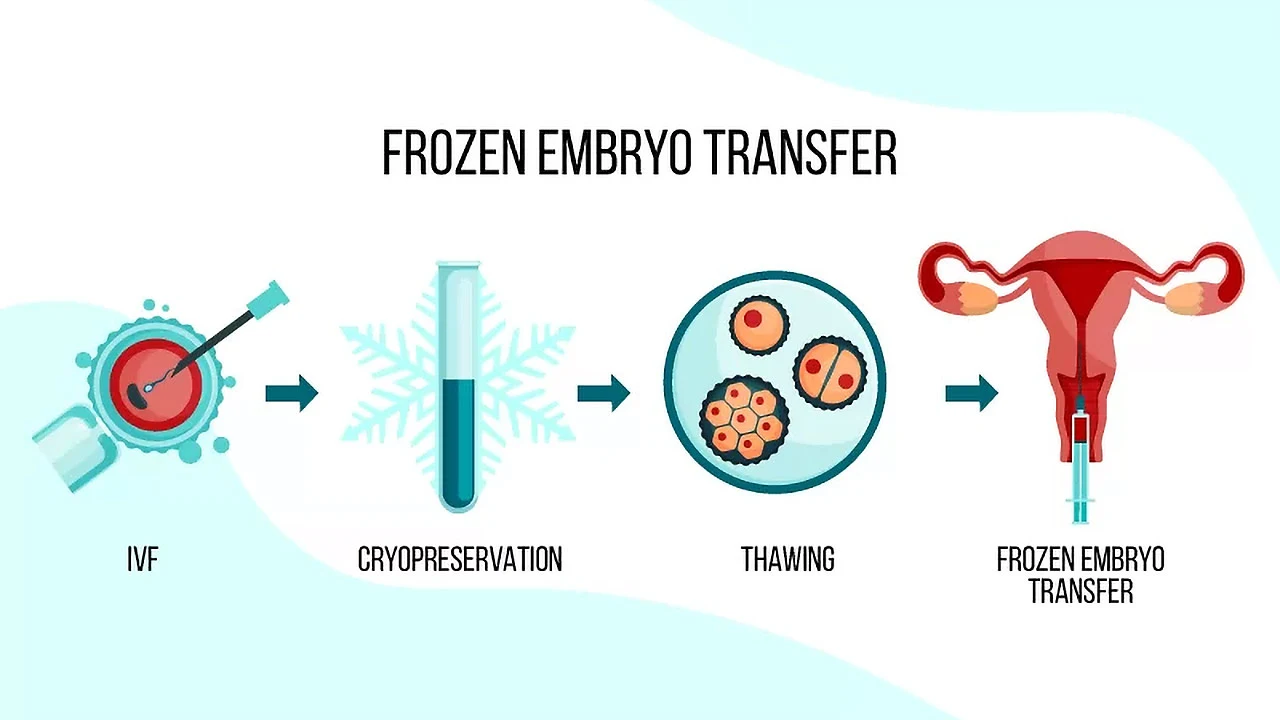
Frozen embryo transfer (FET) is a fertility procedure where previously created and frozen embryos are thawed and placed into the uterus. This comprehensive guide explains the FET process, success rates, benefits, and why it's become a preferred option for many people navigating infertility treatment and building their families.

The vital role of fertility preservation and egg donation in helping women overcome reproductive challenges, allowing them to control their family planning. It highlights how these advancements in reproductive medicine enable women to preserve their fertility and access healthier eggs for future pregnancies.

Egg freezing does not reduce natural fertility or ovarian reserve. This comprehensive guide examines how oocyte cryopreservation works, success rates by age, potential risks including OHSS, costs, and psychological benefits. Facts about preserving reproductive options while maintaining natural conception ability for career-focused and medically indicated fertility preservation.

The best age to freeze sperm and eggs depends on biology, fertility health, and personal choice. Experts recommend egg freezing before 35 and sperm freezing before 40 for stronger outcomes. Advances in technology and lifestyle factors also shape fertility preservation decisions.

Egg freezing allows women to preserve their fertility by extracting, freezing, and storing eggs for future use. Whether postponing parenthood for career, personal reasons, or medical treatments, this comprehensive guide explains the process, costs, success rates, and who should consider this increasingly popular fertility preservation option.

