Home
 ArticlesArticles
ArticlesArticlesMosaic embryos are becoming more common in IVF reports, raising questions about safety, implantation potential, and pregnancy outcomes. This article explains what mosaic embryos are, how PGT-A identifies them, their success rates, and how clinics prioritize transfers, helping patients understand their real possibilities and limitations



People beginning IVF often focus on egg quality, hormones, medications, and embryo grading. But one topic that consistently creates confusion, even among well-informed patients, is mosaic embryos. As preimplantation genetic testing for aneuploidy (PGT-A) is used more often, mosaic embryos are showing up more in lab reports, raising questions about their safety, success rates, and whether they can result in healthy pregnancies. This article breaks down what mosaic embryos are, how they are identified, and why they’ve become a focus of modern reproductive medicine.
Every embryo begins as a single fertilized egg that divides repeatedly. Sometimes, as these early cell divisions occur, errors arise in chromosome number. When only some of the embryo’s cells are affected, the embryo becomes mosaic, containing both normal (euploid) and abnormal (aneuploid) cells.
Such an embryo differs from fully normal embryos (all euploid) or fully abnormal embryos (all aneuploid). Mosaic embryos sit in a gray zone, which is why interpretation is challenging, especially in the context of mosaic embryos and IVF decision-making.

How Mosaic Embryos Are Identified Through PGT-A
PGT-A tests a small sample, typically 5–7 cells, from the embryo’s outer layer (trophectoderm). The inner cell mass, which becomes the baby, is not biopsied. Because mosaicism is uneven, the sample may capture a mixture of normal and abnormal cells.
Clinics classify mosaicism based on the percentage of abnormal signals in the biopsy:
This percentage reflects the biopsy only, not necessarily the entire embryo. That limitation is one of the biggest reasons mosaic embryos require careful interpretation.
A while back, mosaic embryos were often discarded, but today multiple studies indicate that they can implant, lead to ongoing pregnancies, and result in healthy live births. Researchers now know that embryos can fix themselves to some extent, where normal cells might grow faster and outnumber the abnormal ones, abnormal cells might only develop in the placenta, and some abnormal cells might die off on their own. These natural mechanisms help explain why many mosaic embryos behave more like healthy embryos than previously assumed. However, outcomes still vary depending on the type of chromosomal abnormality, the level of mosaicism, the quality of the embryo, and the patient’s medical history. For this reason, clinics avoid using a “one-rule-fits-all” approach.
When counseling patients, clinics consider the most current research and their lab’s performance data. Many now take the view that
When no euploid embryos are available, a common scenario for women over 37 or those with diminished ovarian reserve, mosaic embryos may still offer a meaningful chance at pregnancy.
Fertility specialists typically follow a structured approach:

The Importance of Prenatal Testing After Mosaic Embryo Transfer
If a mosaic embryo is transferred and results in pregnancy, clinics generally recommend:
These steps help ensure that the pregnancy is monitored appropriately. Data so far show that most mosaic-derived pregnancies test normal.
Mosaic embryos were once considered a last-resort option, but today they represent a viable, and occasionally the only, pathway to pregnancy for many patients. They carry uncertainty, but also possibility. Backed by careful counseling and appropriate prenatal testing, mosaic embryo transfers are helping people build families who otherwise might not have had the chance. As science evolves, one message is consistent: mosaicism is not a verdict; it is a spectrum, and many embryos on that spectrum can still lead to healthy babies.
Disclaimer: This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Fertility conditions vary widely, and the technologies and procedures described may not be appropriate for every individual. Always consult a qualified healthcare professional, such as a gynecologist or reproductive endocrinologist, for personalized medical guidance. Never disregard medical advice or delay seeking care because of information presented here.



Advanced female age causes fertility decline through reduced egg quantity, increased chromosomal abnormalities, and mitochondrial dysfunction. Understanding these biological mechanisms helps women make informed family planning decisions. Modern fertility treatments including IVF, preimplantation genetic testing, and egg freezing offer practical solutions to overcome age-related reproductive challenges when trying to conceive.
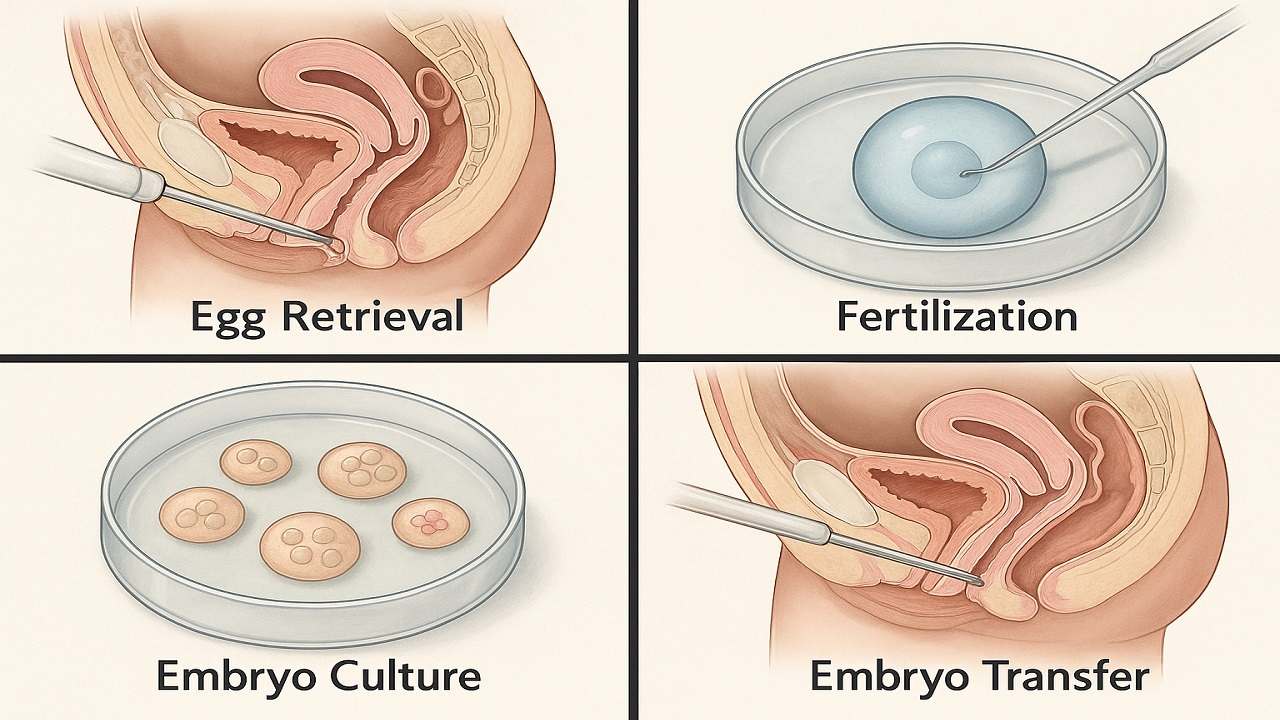
In Vitro Fertilization (IVF) process step by step, emphasising the importance of various stages such as ovarian stimulation, egg retrieval, fertilization, and embryo transfer in maximising the In Vitro Fertilization (IVF) Success Rate. It highlights how a thorough understanding of the procedure can prepare couples and individuals for their In Vitro Fertilization(IVF) journey, ultimately improving their chances of achieving a successful pregnancy.

Vitamin D Deficiency Affect IVF outcomes by influencing endometrial receptivity, embryo quality, and hormone balance. Clinical evidence, age-specific risks, and PCOS implications, while offering actionable strategies to optimize Vitamin D levels and improve IVF success rates and pregnancy outcomes in a structured, patient-focused approach.

Preimplantation Genetic Testing (PGT) revolutionizes IVF by screening embryos for chromosomal abnormalities and genetic disorders before transfer. This advanced technology increases pregnancy success rates, reduces miscarriage risk, prevents inherited diseases, and shortens time to pregnancy while providing diagnostic clarity and reducing emotional stress for couples.

Clinical evidence increasingly demonstrates that emotional stress or grief reduces the chances of IVF success through sophisticated biochemical pathways that directly influence reproductive physiology. This relationship extends far beyond simple correlations, revealing profound mechanistic connections between psychological distress and the delicate orchestration of hormonal events essential for successful conception.
IVF in 2025 is shifting from hype to evidence-based innovation. As precision, automation, AI, and genetic advances reshape fertility care, patients must distinguish proven breakthroughs from outdated add-ons. This guide examines five groundbreaking IVF technologies in 2025 to understand which advances genuinely improve outcomes

Managing Recurrent Implantation Failure (RIF) outlines evidence-based diagnostics and treatment pathways to improve IVF success rates, emphasizing clarity, cautious use of add-ons, and realistic patient expectations.

