Home
 ArticlesArticles
ArticlesArticlesManaging Recurrent Implantation Failure (RIF) outlines evidence-based diagnostics and treatment pathways to improve IVF success rates, emphasizing clarity, cautious use of add-ons, and realistic patient expectations.




Managing Recurrent Implantation Failure requires clear definitions, a disciplined diagnostic pathway, and pragmatic, evidence‑based treatment choices aligned with realistic odds of success. The goal is to move from frustration to strategy clarifying what is known, what remains uncertain, and which interventions genuinely shift live birth outcomes.
“Recurrent implantation failure” is widely used yet inconsistently defined, and that ambiguity matters because it drives testing and treatment decisions. Contemporary expert groups suggest withholding a firm RIF label until at least three failed transfers of euploid blastocysts or an age‑adjusted equivalent of unscreened embryos, after excluding other confounders; true, biologically persistent RIF appears to be uncommon and often overdiagnosed.
A practical, working definition still used in clinics is failure to achieve an ongoing pregnancy after multiple transfers of high‑quality embryos, though consensus statements emphasize euploid embryos as the benchmark when possible. In parallel, clinicians caution that not all IVF failure is “recurrent” or purely an implantation defect male factor, embryo aneuploidy, uterine pathology, and age‑related decline often dominate the odds.
Managing Recurrent Implantation Failure (RIF) begins with reframing: most patients who experience several failed transfers are not destined for persistent failure, and many will conceive with continued standard care, particularly when euploid embryos are available. Keeping this context front‑and‑center tempers anxiety and helps prioritize interventions with demonstrated value.
Patients typically reach a suspected RIF milestone after two to four embryo transfers without an ongoing pregnancy, often following cycles with morphologically “good” embryos. The journey is emotionally charged, and information online ranges from rigorous to speculative; structured evaluation prevents drift into low‑yield testing and unproven add‑ons.
Underlying contributors span embryo competence, uterine environment, and systemic factors. Age‑related aneuploidy remains a leading driver of repeated negative outcomes, while focal uterine issues (polyps, adhesions, submucous fibroids), chronic endometritis, and rare immuno‑thrombotic conditions can play roles; careful triage distinguishes usual risks from true outliers.
For professionals guiding next steps, Managing Recurrent Implantation Failure (RIF) is done by acknowledging uncertainty where it exists while anchoring decisions to high‑quality evidence and consensus recommendations, especially from organizations advancing good‑practice frameworks.
A comprehensive but disciplined work‑up focuses on three pillars: embryo quality, endometrium/uterus, and select systemic factors. The aim is to verify basics first, escalating only when justified by history or findings.
Key elements typically include:
While “immunology panels” are frequently marketed, consensus cautions against broad, non‑specific immune testing absent clear clinical indications, given limited standardization and variable predictive value. Instead, focus on well‑defined entities such as antiphospholipid syndrome in patients with compatible histories or laboratory evidence.
Endometrial receptivity testing, particularly the Endometrial Receptivity Array (ERA), aims to personalize embryo transfer timing based on gene expression and progesterone exposure. The concept is compelling, but multiple cohort studies and a large randomized trial found no improvement in live birth with ERA‑guided transfers in unselected patients undergoing frozen euploid embryo transfer.
Regulatory and advisory bodies have reflected this neutral evidence position, recommending caution about routine use outside specific contexts. For most patients, careful standard timing and luteal support remain appropriate, with ERA considered selectively after meticulous exclusion of other factors.
The immune system’s role in implantation is biologically plausible, but clinical translation remains uneven; many “immune protocols” have limited or conflicting evidence, and costs and side effects can be nontrivial. Network meta‑analysis suggests some experimental immunomodulatory strategies, such as intrauterine PBMCs or PRP may improve clinical pregnancy and, in some analyses, live birth, yet heterogeneity and indirect comparisons warrant caution.
Managing Recurrent Implantation Failure requires communicating that “immune” interventions are best reserved for defined indications or research contexts, not as first‑line solutions after a small number of failed transfers.
Euploidy screening via PGT‑A, when appropriate, reduces the confounding effect of embryo aneuploidy and clarifies whether repeated failures likely reflect uterine or systemic factors. For patients of advanced maternal age or with prior aneuploid losses, prioritizing euploid embryo transfer focuses efforts where they matter.
When repeated euploid transfers fail, attention shifts to subtle uterine factors, transfer technique, and hormone timing; a thorough lab‑clinic review of stimulation parameters, culture conditions, and luteal support is worthwhile, even if major modifiable differences are rare. This is also the juncture where donor embryos may enter the conversation for couples facing persistent embryo quality constraints.
Many patients improve with thoughtful adjustments rather than aggressive overhauls; protocol finesse and transfer execution often deliver more than exotic add‑ons. Interventions should be sequenced from high‑value, low‑risk steps to more selective measures.
Pragmatic options include:
Some clinics may trial intrauterine PRP or PBMC‑based approaches in research‑oriented protocols given meta‑analytic signals, but patients should be advised on evidence uncertainties, costs, and the importance of informed consent. Likewise, any immunomodulation should be indication‑driven rather than reflexive.
A central message in Managing Recurrent Implantation Failure (RIF) is that persistent RIF is rare; most patients’ probability of success remains meaningful, particularly with euploid embryos and correction of any uterine factors. Even after several failed transfers, cumulative live birth rates often climb with continued, standard‑of‑care attempts.
Importantly, psychological support is not ancillary structured counseling helps patients tolerate uncertainty and avoids decision fatigue that can lead to overtesting or therapy shopping. Professional teams should normalize the emotional load while reinforcing evidence‑aligned plans.

An editorially sound pathway begins with definition discipline, proceeds through high‑yield diagnostics, and culminates in tailored adjustments with transparent expectations. This is the essence of managing recurrent implant failure, turning a diffuse label into a structured plan with measurable steps.
When done well, Managing Recurrent Implantation Failure replaces anxiety with structure, affirming that persistent, biologically driven RIF is uncommon, that many patients will succeed with optimized standard care, and that add‑ons should be the exception, not the rule. In this framework, definition discipline, embryo competence, uterine optimization, and cautious application of selective tools deliver the most meaningful improvements in live birth probability and patient experience.



Advanced female age causes fertility decline through reduced egg quantity, increased chromosomal abnormalities, and mitochondrial dysfunction. Understanding these biological mechanisms helps women make informed family planning decisions. Modern fertility treatments including IVF, preimplantation genetic testing, and egg freezing offer practical solutions to overcome age-related reproductive challenges when trying to conceive.
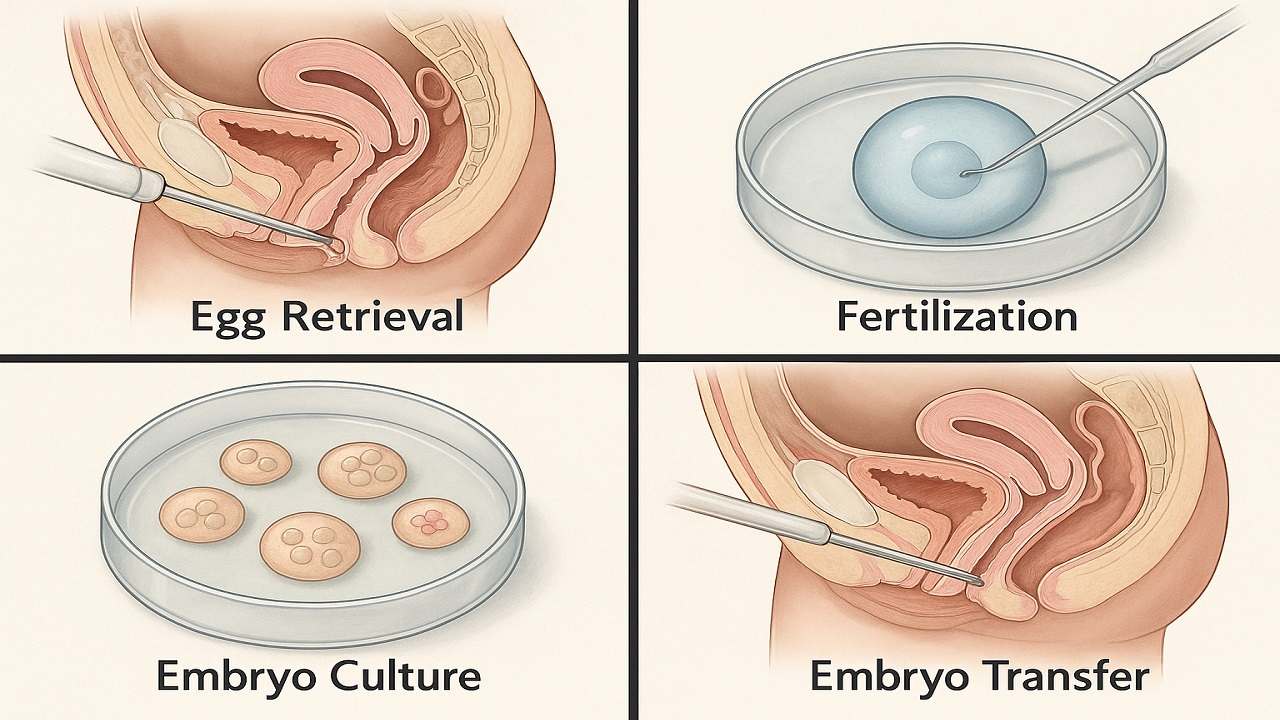
In Vitro Fertilization (IVF) process step by step, emphasising the importance of various stages such as ovarian stimulation, egg retrieval, fertilization, and embryo transfer in maximising the In Vitro Fertilization (IVF) Success Rate. It highlights how a thorough understanding of the procedure can prepare couples and individuals for their In Vitro Fertilization(IVF) journey, ultimately improving their chances of achieving a successful pregnancy.

Vitamin D Deficiency Affect IVF outcomes by influencing endometrial receptivity, embryo quality, and hormone balance. Clinical evidence, age-specific risks, and PCOS implications, while offering actionable strategies to optimize Vitamin D levels and improve IVF success rates and pregnancy outcomes in a structured, patient-focused approach.

Preimplantation Genetic Testing (PGT) revolutionizes IVF by screening embryos for chromosomal abnormalities and genetic disorders before transfer. This advanced technology increases pregnancy success rates, reduces miscarriage risk, prevents inherited diseases, and shortens time to pregnancy while providing diagnostic clarity and reducing emotional stress for couples.

Clinical evidence increasingly demonstrates that emotional stress or grief reduces the chances of IVF success through sophisticated biochemical pathways that directly influence reproductive physiology. This relationship extends far beyond simple correlations, revealing profound mechanistic connections between psychological distress and the delicate orchestration of hormonal events essential for successful conception.
IVF in 2025 is shifting from hype to evidence-based innovation. As precision, automation, AI, and genetic advances reshape fertility care, patients must distinguish proven breakthroughs from outdated add-ons. This guide examines five groundbreaking IVF technologies in 2025 to understand which advances genuinely improve outcomes

