Home
 ArticlesArticles
ArticlesArticlesThe significant role of the female immune system in influencing IVF outcomes. It discusses how immune health affects ovarian function, embryo recognition, implantation success, and pregnancy risks. The relationship between hormonal fluctuations, inflammation, and psychosocial stress is explored, along with future interventions tailored to immune health in IVF.




In the delicate realm of reproductive medicine, few questions are as compelling as how the human immune system influences fertility treatments. When a woman undergoes in vitro fertilization (IVF), countless biological interactions shape the final outcome, and her immune health is a central player. Often overlooked in favour of hormones and egg quality, immunity acts as both a gatekeeper and a guide, determining whether conception and implantation can occur successfully. To understand this connection, one must explore how immunity influences ovarian function, embryo recognition, implantation, and ultimately pregnancy.
Contrary to the notion that the immune system simply “protects”, reproductive science reveals it also must “tolerate”. A woman’s body must strike a balance: defending against harmful infections while simultaneously allowing the embryo a unique genetic blend of both parents to implant and grow. This is particularly critical during IVF, where the process bypasses natural selection mechanisms. Subtle immune imbalances, such as overactive natural killer (NK) cells or miscommunication between immune regulators, may compromise embryo acceptance and hinder implantation.
Recent studies published in Reproductive Immunology highlight that women with autoimmune conditions or heightened immune activation face lower IVF success rates. This underlines the fact that a woman’s immune system influences IVF treatment outcomes not in isolation, but as part of a broader, intricate network of reproductive health.

Hormones and immunity are deeply intertwined. Estrogen and progesterone, both central to IVF cycles, regulate immune activity within the uterus. Progesterone, often called the “pregnancy hormone”, promotes a more tolerant immune environment that allows the embryo to attach without being perceived as foreign. If progesterone signalling falters, immune cells may become overactive, leading to implantation failure or an early miscarriage.
Cortisol, another key player, illustrates the same point from a different angle. Stress-induced immune responses may disrupt hormonal cycles and affect ovarian stimulation. This interplay demonstrates that IVF success requires more than hormonal supplementation it requires immune equilibrium.
The ovaries are not immune-isolated. Cytokines, small proteins secreted by immune cells, play essential roles in follicular development and egg maturation. A study in Fertility and Sterility revealed that abnormal cytokine levels correlate with reduced ovarian response during IVF stimulation. Women with underlying inflammatory disorders often produce eggs of lower quality, which may compromise embryo viability.
This is where lifestyle factors, like diet, sleep, and even stress management, can directly modulate immune behaviour. Anti-inflammatory diets and healthier metabolic balance are increasingly viewed as adjunctive strategies for women undergoing IVF.
The early embryo is an immunological paradox. It carries paternal antigens unfamiliar to the mother’s body, yet it must be protected rather than rejected. Therefore, the maternal immune system must adapt, facilitating "crosstalk" with the embryo via signalling molecules. Poor communication, particularly involving regulatory T-cells, has been associated with recurrent IVF failures.
In some cases, immune-related imbalances manifest as higher rates of embryo fragmentation or impaired blastocyst development. Such findings reinforce the idea that a woman’s immune system influences IVF treatment outcomes long before implantation even begins.
Perhaps the most critical stage where immunity intervenes is implantation. The uterine lining, or endometrium, must undergo controlled immune remodelling to allow embryo adhesion. NK cells, though often misunderstood, are not purely destructive. In healthy pregnancies, they promote vascular development essential for supporting the embryo. However, if they become hyperactive, they may instead impede implantation.
Clinicians have investigated targeted therapies such as intralipid infusions or corticosteroids to moderate immune hyperactivity in women with repeated IVF failures. While evidence remains mixed, these emerging approaches reflect growing recognition that immune misregulation can derail IVF even when embryos are genetically normal.
Even after successful implantation, immune imbalances continue to shape outcomes. Overactive immune responses have been linked to complications such as preeclampsia, gestational diabetes, and recurrent miscarriage. Autoimmune disorders like lupus or thyroiditis present heightened risks during IVF, requiring close monitoring and often immunosuppressive strategies to protect pregnancy.
Notably, inflammation driven by obesity also ties into these risks. Excess adipose tissue acts as an immune organ in itself, releasing cytokines that may undermine both embryo quality and placental development. Thus, immune health is not an isolated parameter but part of the broader metabolic and systemic well-being of the patient.
It is impossible to ignore the mind-body connection in IVF. The emotional tolls of infertility and treatment cycles can shift immune behaviours through stressful pathways. Elevated cortisol and inflammatory markers correlate with reduced implantation rates, showing how psychological strain translates into biological disruption.
Supportive counselling, mindfulness practices, and stress-reduction techniques are increasingly recommended not only for emotional resilience but also for their tangible impact on immune balance during IVF.
The future of assisted reproduction may well hinge on immunological personalisation. Precision medicine approaches are investigating immune profiling to tailor IVF protocols. For example, pre-IVF testing for NK cell activity or cytokine imbalances could help clinicians design targeted therapies. Trials are exploring biologics, such as anti-TNF agents, to control inflammation in women with repeated implantation failure.
Equally promising are non-pharmacological innovations. Lifestyle interventions, personalised nutrition, and microbiome modulation are all being studied as ways to shape immune behaviours in favour of reproduction. In short, tomorrow’s IVF may not be standardised, but it may be immune-informed.
The story of IVF is not only about eggs, sperm, and embryos; it is equally about the environment into which life is invited. The evidence is clear that a woman’s immune system influences IVF treatment outcomes at every stage, from ovarian stimulation to implantation and pregnancy maintenance. Balancing defence and tolerance, the immune system is at once protector and potential adversary. For patients and clinicians alike, recognising this influence transforms IVF from a purely mechanical intervention into a holistic process, one where immunity, lifestyle, and emotional resilience are woven together in the pursuit of new beginnings.



Advanced female age causes fertility decline through reduced egg quantity, increased chromosomal abnormalities, and mitochondrial dysfunction. Understanding these biological mechanisms helps women make informed family planning decisions. Modern fertility treatments including IVF, preimplantation genetic testing, and egg freezing offer practical solutions to overcome age-related reproductive challenges when trying to conceive.
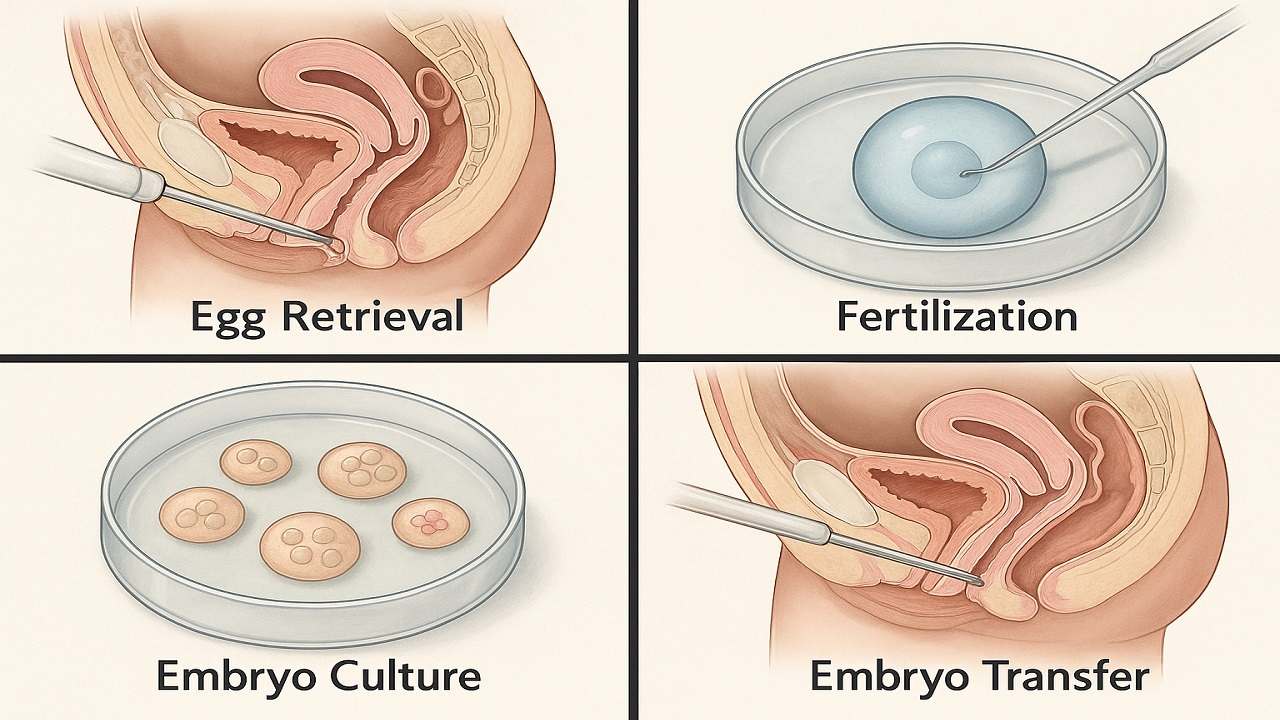
In Vitro Fertilization (IVF) process step by step, emphasising the importance of various stages such as ovarian stimulation, egg retrieval, fertilization, and embryo transfer in maximising the In Vitro Fertilization (IVF) Success Rate. It highlights how a thorough understanding of the procedure can prepare couples and individuals for their In Vitro Fertilization(IVF) journey, ultimately improving their chances of achieving a successful pregnancy.

Vitamin D Deficiency Affect IVF outcomes by influencing endometrial receptivity, embryo quality, and hormone balance. Clinical evidence, age-specific risks, and PCOS implications, while offering actionable strategies to optimize Vitamin D levels and improve IVF success rates and pregnancy outcomes in a structured, patient-focused approach.

Preimplantation Genetic Testing (PGT) revolutionizes IVF by screening embryos for chromosomal abnormalities and genetic disorders before transfer. This advanced technology increases pregnancy success rates, reduces miscarriage risk, prevents inherited diseases, and shortens time to pregnancy while providing diagnostic clarity and reducing emotional stress for couples.

Clinical evidence increasingly demonstrates that emotional stress or grief reduces the chances of IVF success through sophisticated biochemical pathways that directly influence reproductive physiology. This relationship extends far beyond simple correlations, revealing profound mechanistic connections between psychological distress and the delicate orchestration of hormonal events essential for successful conception.
IVF in 2025 is shifting from hype to evidence-based innovation. As precision, automation, AI, and genetic advances reshape fertility care, patients must distinguish proven breakthroughs from outdated add-ons. This guide examines five groundbreaking IVF technologies in 2025 to understand which advances genuinely improve outcomes

Managing Recurrent Implantation Failure (RIF) outlines evidence-based diagnostics and treatment pathways to improve IVF success rates, emphasizing clarity, cautious use of add-ons, and realistic patient expectations.

