Home
 ArticlesArticles
ArticlesArticlesThe IVF effects on breastfeeding, exploring hormonal, anatomical, and psychosocial factors. It reviews clinical evidence and infant outcomes.




Advances in assisted reproductive technologies have brought hope to countless families wishing to conceive. Yet as more infants are born via in vitro fertilization (IVF), questions naturally arise about whether conception methods influence the earliest stages of nurturing and nutrition, chief among them breastfeeding. Understanding the IVF effects on breastfeeding is vital for healthcare professionals and parents alike, ensuring that all infants, regardless of conception route, achieve optimal growth, bonding, and long-term health outcomes.
Breastfeeding success hinges on complex hormonal, anatomical, and psychosocial elements. Prolactin and oxytocin drive milk synthesis and ejection, while infant suckling stimulates a reinforcing feedback loop. Maternal health, parity, stress levels, and support systems also shape lactation trajectories. In the context of IVF, the central concern is whether ovulation induction protocols, embryo manipulation, or hormonal milieu perturb these finely tuned processes.
 Hormonal Stimulation and Postpartum Milk Supply
Hormonal Stimulation and Postpartum Milk SupplyDuring IVF, women often undergo controlled ovarian hyperstimulation with gonadotropins and may receive progesterone or estrogen supplementation to support early pregnancy. Theoretical concerns suggest that elevated exogenous hormones could desensitise mammary receptors or disrupt endogenous prolactin secretion postpartum. However, clinical observations indicate that most postpartum hormone levels normalise swiftly, and studies find no consistent difference in colostrum volume or mature milk onset between IVF and naturally conceived mothers. Thus, IVF effects on breastfeeding via hormonal carryover appear minimal.
Percutaneous oocyte retrieval involves transvaginal needle aspiration under ultrasound guidance, leaving no direct interference with mammary tissue. Furthermore, caesarean delivery rates are sometimes higher in IVF pregnancies, but surgical incision on the abdomen exerts little influence on breast development or function. Clinical data show comparable breast engorgement patterns and nipple-areolar complex integrity among mothers regardless of conception history, underscoring that procedural aspects of IVF do not compromise anatomical prerequisites for effective nursing.
Emotional well-being significantly shapes breastfeeding outcomes. IVF journeys can entail heightened anxiety, prolonged waiting, and financial stress, potentially undermining maternal confidence in early postpartum self-efficacy. Yet, many mothers who conceive through IVF report profound gratitude and determination, channelling their emotional investment into diligent breastfeeding efforts. While some studies describe marginally lower exclusive breastfeeding rates at hospital discharge among IVF mothers, often linked to initial stress or medical complications, these differences typically dissipate by six weeks postpartum with proper lactation support.
Infants conceived via IVF carry a slightly elevated risk of preterm birth and low birth weight, factors known to challenge breastfeeding initiation. Premature infants may exhibit immature suck-swallow coordination, necessitating supplemental tube or pump-expressed feeds. Here, the IVF effects on breastfeeding are indirect: infants’ medical status, rather than the IVF procedure itself, dictates feeding method. Enhanced neonatal care protocols and kangaroo mother care have, however, demonstrated robust success in transitioning these infants to direct breastfeeding, achieving rates on par with term peers by discharge.
Mothers undergoing IVF may take antenatal medications like low-dose aspirin, heparin for thrombophilia, or thyroid supplements that raise questions about drug passage into breast milk. Extensive pharmacokinetic research confirms that most standard IVF adjuncts exist in milk at negligible levels, posing no known risk to infants. Even progesterone administered for luteal support has high molecular weight and minimal oral bioavailability in the neonate. Therefore, the effects of IVF on breastfeeding from medication exposures are generally reassuring, with breast milk remaining the optimal first food.
Breastfeeding conveys immunological protection and supports neurodevelopment through bioactive factors and long-chain fatty acids. Comparative studies tracking growth and cognitive milestones reveal no discernible gaps between breastfed infants of IVF and naturally conceived cohorts. Indeed, because IVF parents often receive more intensive prenatal education and follow-up care, they may access lactation consultants earlier and maintain exclusive breastfeeding longer. Consequently, when normalised for socioeconomic variables, the IVF effects on breastfeeding appear neutral or even slightly favourable regarding infant outcomes.
Ensuring breastfeeding success involves proactive measures both prenatally and postpartum. Healthcare teams can:
By weaving these practices into standard IVF protocols, clinicians can mitigate indirect barriers and optimise IVF's effects on breastfeeding for all families.
The landscape of reproductive medicine continually evolves, and emerging investigations are probing subtle epigenetic and microbiome influences of conception methods on neonatal and maternal health. Longitudinal cohorts tracking breastfeeding duration, milk composition, and infant microbiota will refine our understanding of whether in vitro conditions leave any lasting imprint. Personalised reproductive care, integrating genomic, metabolic, and psychosocial profiling, promises to tailor breastfeeding support strategies to women who conceive through IVF, further minimising any potential intervention gaps.
Current evidence indicates that in vitro fertilisation alone has a negligible direct impact on breastfeeding physiology or milk safety. Observed variations in early lactation typically stem from associated obstetric or neonatal complications rather than the IVF process. By recognising and addressing these indirect factors, particularly preterm birth challenges and maternal stress, healthcare providers can ensure that all mothers, regardless of conception route, achieve their breastfeeding goals. Embracing a holistic, multidisciplinary approach will safeguard the earliest nourishment and bonding experiences, ensuring that IVF effects on breastfeeding remain a topic of reassurance rather than concern.



Advanced female age causes fertility decline through reduced egg quantity, increased chromosomal abnormalities, and mitochondrial dysfunction. Understanding these biological mechanisms helps women make informed family planning decisions. Modern fertility treatments including IVF, preimplantation genetic testing, and egg freezing offer practical solutions to overcome age-related reproductive challenges when trying to conceive.
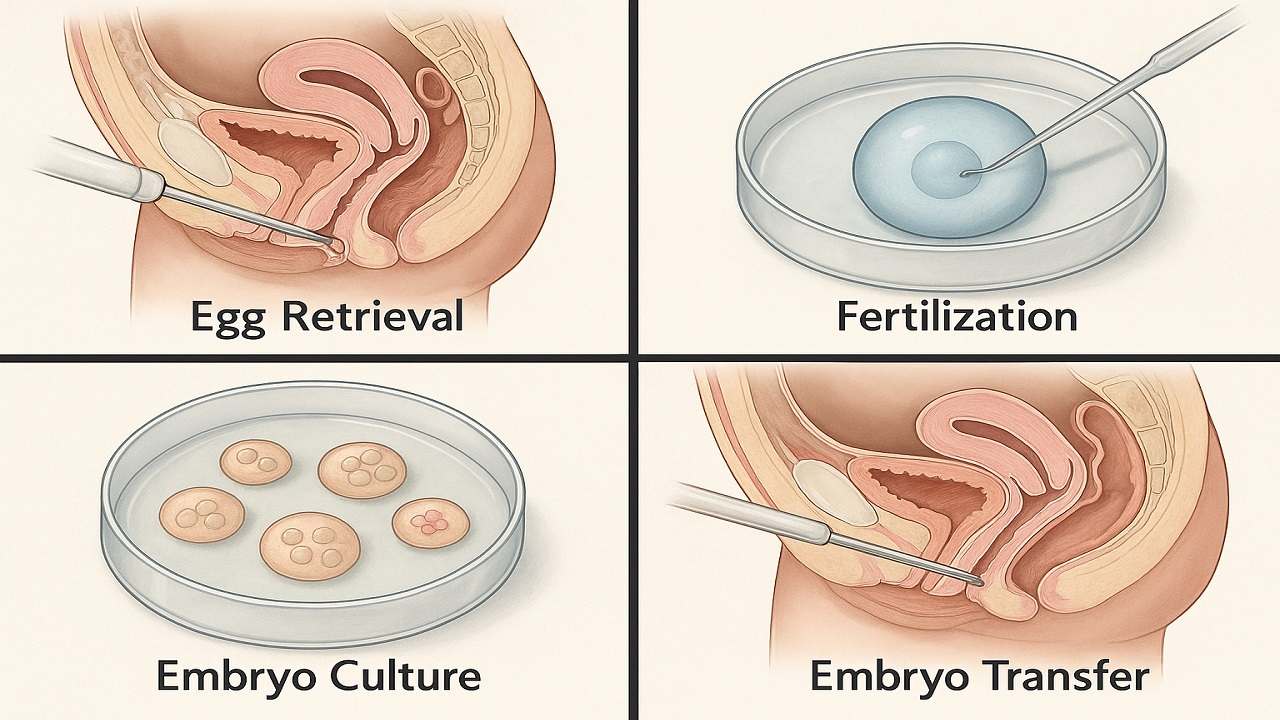
In Vitro Fertilization (IVF) process step by step, emphasising the importance of various stages such as ovarian stimulation, egg retrieval, fertilization, and embryo transfer in maximising the In Vitro Fertilization (IVF) Success Rate. It highlights how a thorough understanding of the procedure can prepare couples and individuals for their In Vitro Fertilization(IVF) journey, ultimately improving their chances of achieving a successful pregnancy.

Vitamin D Deficiency Affect IVF outcomes by influencing endometrial receptivity, embryo quality, and hormone balance. Clinical evidence, age-specific risks, and PCOS implications, while offering actionable strategies to optimize Vitamin D levels and improve IVF success rates and pregnancy outcomes in a structured, patient-focused approach.

Preimplantation Genetic Testing (PGT) revolutionizes IVF by screening embryos for chromosomal abnormalities and genetic disorders before transfer. This advanced technology increases pregnancy success rates, reduces miscarriage risk, prevents inherited diseases, and shortens time to pregnancy while providing diagnostic clarity and reducing emotional stress for couples.

Clinical evidence increasingly demonstrates that emotional stress or grief reduces the chances of IVF success through sophisticated biochemical pathways that directly influence reproductive physiology. This relationship extends far beyond simple correlations, revealing profound mechanistic connections between psychological distress and the delicate orchestration of hormonal events essential for successful conception.
IVF in 2025 is shifting from hype to evidence-based innovation. As precision, automation, AI, and genetic advances reshape fertility care, patients must distinguish proven breakthroughs from outdated add-ons. This guide examines five groundbreaking IVF technologies in 2025 to understand which advances genuinely improve outcomes

Managing Recurrent Implantation Failure (RIF) outlines evidence-based diagnostics and treatment pathways to improve IVF success rates, emphasizing clarity, cautious use of add-ons, and realistic patient expectations.

