Home
 ArticlesArticles
ArticlesArticlesWhether women with breast cancer can undergo IVF safely, focusing on clinical risks, hormonal changes, fertility preservation strategies, and emerging research supporting motherhood after cancer treatment.




For decades, breast cancer was considered an inevitable thief of a woman’s reproductive future. Treatment urgency often left little room for fertility conversations, and the idea of conceiving through assisted reproduction was met with hesitation. Today, however, advances in reproductive medicine and oncology have reshaped this outlook. Increasingly, physicians and patients alike ask, Can women with breast cancer undergo IVF safely?
The answer is layered, sitting at the intersection of clinical caution, hormonal science, and human aspiration. On one hand, cancer therapies like chemotherapy and radiation impair ovarian reserve, threatening future fertility. On the other hand, in-vitro fertilization (IVF) offers a chance at biological motherhood but raises concerns about estrogen exposure, recurrence risk, and timing relative to treatment. This delicate balance makes the discussion not only a medical consideration but also an ethical and emotional one.

One of the foremost worries surrounding IVF in breast cancer patients is hormone sensitivity. Estrogen-receptor positive tumours, which account for nearly two-thirds of breast cancers, thrive in estrogen-rich environments. Standard IVF protocols often involve high doses of gonadotropins, elevating estrogen levels dramatically a red flag for oncologists.
To address this, fertility specialists now employ modified ovarian stimulation protocols. Medications like letrozole or tamoxifen are incorporated to suppress estrogen levels while still allowing multiple eggs to mature. Clinical trials, including large-scale studies from Memorial Sloan Kettering and European reproductive centres, have shown that such tailored protocols do not increase recurrence risk in the short to medium term.
Timing is everything. Fertility preservation must be carefully synchronised with cancer therapy without compromising survival outcomes. IVF cycles typically take two to three weeks, which can be safely accommodated before starting chemotherapy in many cases. For patients requiring immediate treatment, experimental options such as ovarian tissue cryopreservation may serve as alternatives.

The positive trial (Pregnancy Outcome and Safety of Interrupting Therapy for Women with Endocrine-Responsive Breast Cancer) has further illuminated this space. Early findings suggest that pausing endocrine therapy to attempt pregnancy or undergo IVF does not significantly worsen cancer outcomes, provided treatment resumes afterward. While long-term results are still awaited, this represents a monumental shift toward patient-centred care.
The success rates of IVF among breast cancer survivors can be influenced by several factors, including age at diagnosis, treatment intensity, and ovarian reserve being the primary ones.ry ones. Chemotherapy, particularly alkylating agents, accelerates ovarian ageing, leading to diminished ovarian response. Survivors may yield fewer eggs, and embryo quality may be compromised compared to peers without a cancer history.
Yet, encouragingly, studies from Sweden and the U.S. have demonstrated that live birth rates in survivors undergoing IVF are not markedly different when eggs or embryos were preserved prior to cancer treatment. This suggests that early fertility counselling and preservation can significantly improve outcomes.
For many women, confronting both cancer and infertility is a dual blow to identity, self-image, and future planning. The decision to pursue IVF is not purely medical but deeply emotional. Survivorship studies highlight that women who had access to fertility preservation reported greater long-term quality of life, less decisional regret, and improved psychosocial adjustment.
Still, fears linger, concerns about passing on genetic predispositions, the health of future pregnancies, and whether motherhood could compromise personal survival. Comprehensive counselling by multidisciplinary teams, including oncologists, reproductive specialists, and psychologists, is thus critical.
Research continues to expand options for women with breast cancer seeking IVF. Some promising interventions include:
These innovations reflect the growing alignment between oncology and reproductive medicine, turning fertility preservation into a standard of care rather than an afterthought.
Ultimately, the question, Can women with breast cancer undergo IVF safely? cannot be answered with a blanket yes or no. It is a decision shaped by cancer subtype, treatment stage, patient age, and personal priorities. While risks exist, particularly regarding hormone-sensitive disease, modern reproductive techniques and emerging evidence suggest IVF can be pursued with careful safeguards.
For many, the ability to preserve fertility or achieve motherhood after cancer offers not just biological continuity but profound psychological healing. It is a testament to the resilience of women who refuse to let illness define their future.
The intersection of breast cancer and fertility once seemed fraught with insurmountable barriers. Yet today, science and compassion have carved new paths forward. Can women with breast cancer undergo IVF safely? Increasingly, the evidence says yes with tailored protocols, thoughtful timing, and multidisciplinary support.
This convergence of oncology and reproductive medicine does more than preserve fertility; it restores choice, autonomy, and hope to women navigating one of life’s most difficult journeys. And in that restoration lies not just survival, but renewal.



Advanced female age causes fertility decline through reduced egg quantity, increased chromosomal abnormalities, and mitochondrial dysfunction. Understanding these biological mechanisms helps women make informed family planning decisions. Modern fertility treatments including IVF, preimplantation genetic testing, and egg freezing offer practical solutions to overcome age-related reproductive challenges when trying to conceive.
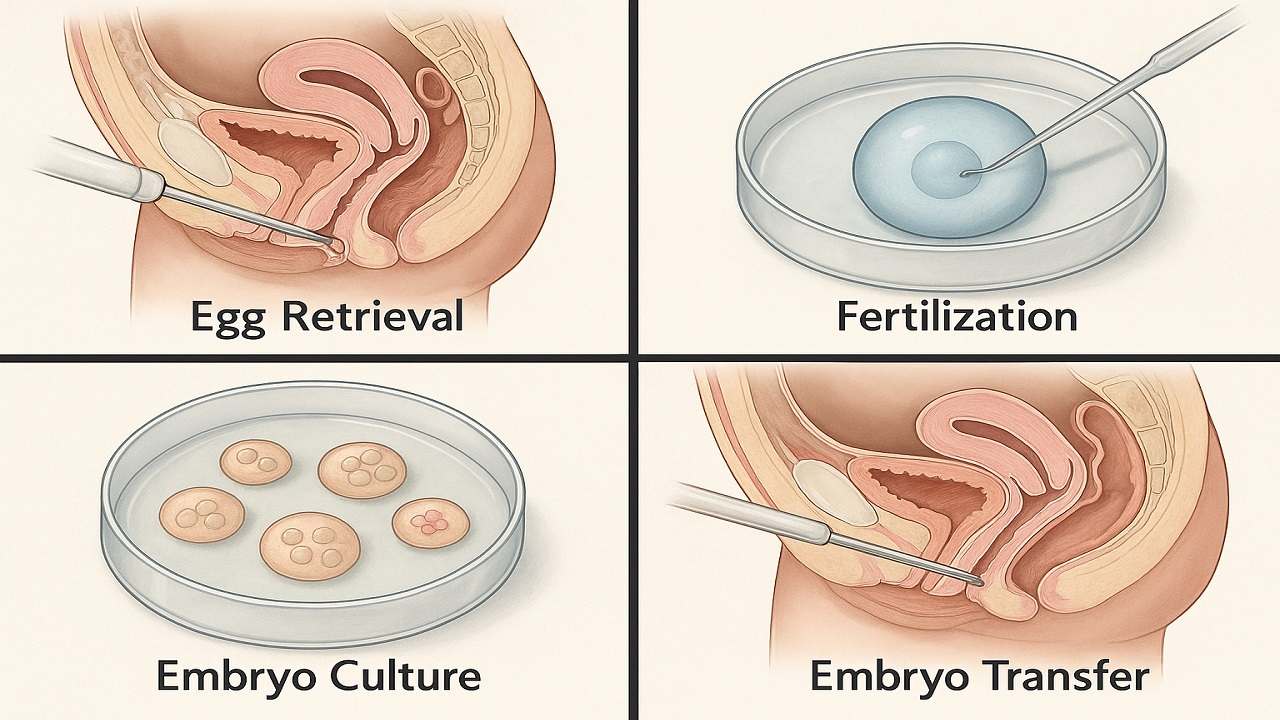
In Vitro Fertilization (IVF) process step by step, emphasising the importance of various stages such as ovarian stimulation, egg retrieval, fertilization, and embryo transfer in maximising the In Vitro Fertilization (IVF) Success Rate. It highlights how a thorough understanding of the procedure can prepare couples and individuals for their In Vitro Fertilization(IVF) journey, ultimately improving their chances of achieving a successful pregnancy.

Vitamin D Deficiency Affect IVF outcomes by influencing endometrial receptivity, embryo quality, and hormone balance. Clinical evidence, age-specific risks, and PCOS implications, while offering actionable strategies to optimize Vitamin D levels and improve IVF success rates and pregnancy outcomes in a structured, patient-focused approach.

Preimplantation Genetic Testing (PGT) revolutionizes IVF by screening embryos for chromosomal abnormalities and genetic disorders before transfer. This advanced technology increases pregnancy success rates, reduces miscarriage risk, prevents inherited diseases, and shortens time to pregnancy while providing diagnostic clarity and reducing emotional stress for couples.

Clinical evidence increasingly demonstrates that emotional stress or grief reduces the chances of IVF success through sophisticated biochemical pathways that directly influence reproductive physiology. This relationship extends far beyond simple correlations, revealing profound mechanistic connections between psychological distress and the delicate orchestration of hormonal events essential for successful conception.
IVF in 2025 is shifting from hype to evidence-based innovation. As precision, automation, AI, and genetic advances reshape fertility care, patients must distinguish proven breakthroughs from outdated add-ons. This guide examines five groundbreaking IVF technologies in 2025 to understand which advances genuinely improve outcomes

Managing Recurrent Implantation Failure (RIF) outlines evidence-based diagnostics and treatment pathways to improve IVF success rates, emphasizing clarity, cautious use of add-ons, and realistic patient expectations.

